


Review
Three cases
·First case
Solitaire & Atlas stents assisted coiling of an ACOM aneurysm
·病例1



Figure 2 GIF. Right ICA angiograms after left ICA compression depicted an un-developed right A1 segment. Rotational DSA and 3D constructions revealed an irregular anterior communicating artery aneurysm.
图 2 GIF. 左侧颈内动脉压颈后右侧颈内动脉造影示右侧A1段不发育。旋转DSA及3D重建证实前交通不规则动脉瘤。
1
Strategy
1.The irregular (triple lobe ) anterior communicating artery aneurysm with multiple daughter sacs had a high rupture risk.
2.The contralateral A1 was undeveloped, which indicates that the anterior communicating artery must be preserved.
3.The aneurysm mainly involved left-A2. Stent-assisted coiling is preferred to remodel the parent artery and decrease the recurrence rate. Therefore the first Solitaire stent was deployed from left A2 to A1. Meanwhile another stent microcatheter was navigated into the right A2 for a second stent, also can provide protection of right A2 during the embolization of AN. Finally, depending on the embolization effect, we decided to deploy 2nd stent or not.
3.动脉瘤主要累及左侧A2,第一枚支架自左侧A2段至A1段释放,选用Solitaire改变成角,以降低复发风险;右侧A2段预先将支架微导管到位,以备第二枚支架的置入,且在动脉瘤栓塞过程中提供保护,最终根据栓塞效果决定是否置入第二枚支架。
2
Operation
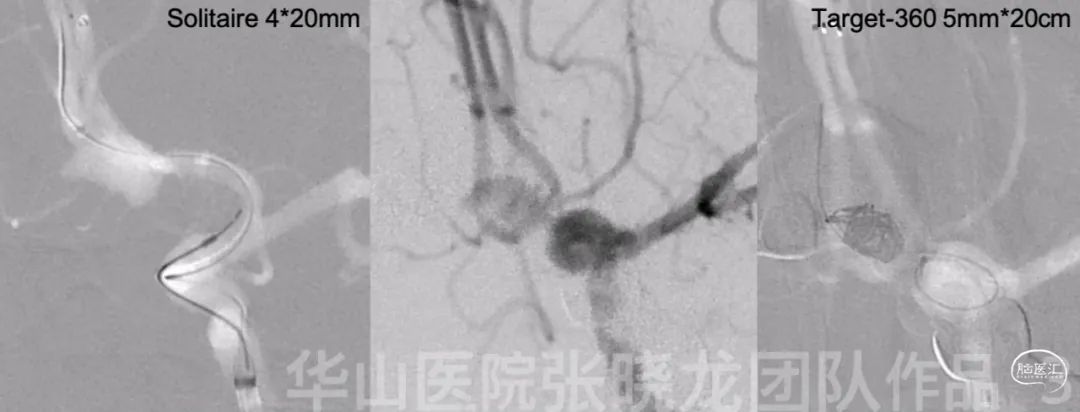
图 3. 测量:动脉瘤大小6.99*4.89mm,瘤颈2.5mm;近端载瘤动脉直径2.2mm,远端左侧载瘤动脉直径2.2mm,远端右侧载瘤动脉直径2.1mm。将6F Envoy DA导引导管置于海绵窦段,Prowler Plus和SL-10微导管头端塑C弯后分别超选至左侧A2及右侧A2段。Solitaire 4*20mm支架置于左侧大脑前动脉A2-1段,覆盖瘤颈。撤出Prowler Plus并调整SL-10微导管于右侧A2段,Echelon-10直头微导管在微导丝引导下进入动脉瘤腔。然后置入Target 360 5mm*20cm弹簧圈。



图 5 GIF. 经导引导管共注入替罗非班15ml及尼莫地平1ml。等待10min后复查造影,动脉瘤未见显影,颅内血管显影良好。

Single stent assisted coiling of an ACOM aneurysm.
·病例2


图 7 GIF. DSA证实前交通动脉瘤,动脉瘤重要累及前交通及左侧大脑前动脉。按压左侧颈内动脉后行造影,右侧A1不发育。
3
Strategy
1.Contralateral A1 segment did not develop, so the anterior communicating artery must be preserved.
2.The aneurysm mainly incorporated the left A2, therefore the first stent should be deployed into the left A2 segment.
3.A SL-10 microcatheter was navigated into the contralateral A2 segment for the second stent.
1.对侧A1段不发育,所以前交通动脉必须保护。
3.同时将SL-10微导管超选至右侧A2段,以备第二枚支架的释放。
4
Operation



Figure 10. The parent artery angle straightened.
图 10. 载瘤动脉成角拉直。
·Third caseDual Solitaire stents assisted coiling of an ACOM aneurysm.
·病例3
一例双支架辅助弹簧圈栓塞前交通动脉瘤。



图 12 GIF. 造影示右侧A1段纤细,右侧颈内动脉颈段小夹层。造影及3D重建证实左侧不规则前交通动脉瘤。
5
Strategy
1.The irregular anterior communicating artery aneurysm with daughter sacs indicating a high rupture risk was suggested treated.
2.The aneurysm wide neck incorporated anterior communicating artery and left A2 segment, while the right A1 was underdeveloped. Therefore the anterior communicating artery must be preserved.
3.Dual Solitaire stents with a Y configuration assisted coiling can be adopted because of a large left A1.4.Stent-induced straightening of the parent arteries combined with a large coil technique can decrease the recurrence rate.
5.Different working projections should be selected for microcatheter navigation, stenting, and coiling.
1.前交通不规则动脉瘤伴子瘤,破裂风险高,建议治疗。
2.前交通宽颈动脉瘤,动脉瘤累及左侧A2段及前交通动脉,右侧A1段发育不佳,所以前交通动脉需要保护。
3.左侧A1段粗大,所以采用双Solitaire “Y”型支架辅助栓塞。
4.支架拉直载瘤动脉成角联合大圈技术,降低动脉瘤复发。
5.选用多个工作角度用于微导管超选、支架释放和栓塞动脉瘤。
6
Operation


Figure 14. Partially inserted Target 360 5mm*10cm coil via an Echelon-10 microcatheter and deployed another Solitaire 4*20mm stent from left A2 to left A1 segment. Then continued the previous coil and the following 5 coils (Target 360 4mm*8cm, 3mm*6cm (*3) and 3mm*8cm).
图 14. 经Echelon-10微导管填入Target 360 5mm*10cm部分弹簧圈袢突入载瘤动脉,Solitaire 4*20mm支架于左侧A2段至瘤颈释放。经微导管继续填入前一枚Target 360 5mm*10cm弹簧圈,及Target 360 4mm*8cm、3mm*6cm (*3)和3mm*8cm弹簧圈。

Figure 15 GIF. Angiograms showed the aneurysm was packed satisfactorily and intracranial vessels were intact.

Figure 16. The parent arteries straightened significantly.
视频 1. 7个月随访造影动脉瘤未见复发。
7
Summary
1.Anterior communicating artery must be preserved for an anterior communicating artery aneurysm with one side anterior cerebral artery un/under-developed. Stents with "Y” or “T”configuration were adopted for preserving anterior communicating artery if an anterior communicating artery aneurysm involved both anterior communicating artery and an A2 segment.
2.In order to decrease infarction events, two microcatheters at most into guiding catheter was suggested. Two stent microcatheters were positioned into bilateral A2 respectively, then retrieving a microcatheter after deploying a stent. Another microcatheter was navigated into the sac for embolization.
3.First stent was deployed from the mainly incorporated side. A second stent can not be deployed if the aneurysm with a relative narrow neck after the first stent deployed.
4.Solitaire was representative of straightening parent artery and low thrombosis.
5.First coil should be selected large. 3D framing coils are preferred for irregular aneurysms.
1.一侧大脑前动脉不发育或发育不佳的前交通动脉瘤,必须保护前交通动脉。如果前交通动脉瘤累及前交通动脉及一侧A2段,需要采用多支架(”Y”或”T”型)技术保护前交通动脉。
2.双支架导管到位,释放一枚支架,撤出该微导管,栓塞微导管到位,然后进行栓塞或释放第二枚支架后栓塞,保证导引导管内只有两根微导管,减少血栓事件。
3.先释放动脉瘤累及较多一侧的支架。若第一枚支架释放后,动脉瘤相对窄颈,第二枚支架可不释放。
4.Solitaire支架载瘤动脉拉直效应明显,且致栓性低。
5.首圈选用大圈成篮,弹簧圈不易压缩;不规则动脉瘤,3D弹簧圈更有利于成篮。

张晓龙
复旦大学附属华山医院
复旦大学附属华山医院放射科主任医师,博士、教授、博士生导师;
斯坦福大学医学院客座临床教授;
主持国家自然科学基金3项,第一作者或通讯作者发表国内外权威期刊文章50余篇;
中华医学会、放射学会、卫生部医政司等组织中担任副主任委员、组长等职务.《中国名医百强榜》神经介入专业中国十强(2012年度、2013年度、2014年度、2015-16年度、2017-18年度);
擅长复杂和疑难脑血管疾病的介入治疗,如复杂脑动脉瘤的栓塞,硬脑膜动静脉瘘栓塞,脑动静脉畸形栓塞,脑梗死的支架,脊髓血管畸形治疗;
自1995年开始从事脑血管疾病介入诊治工作和研究,师从黄祥龙教授、沈天真教授和凌锋教授,是我国最早从事神经介入的专家之一。2010年9月至今连续介入治疗颅内动脉瘤1500余例,无操作致死.

点击或扫描上方二维码
查看更多“介入”内容
