


Case Review
• 68 y/o male.
• Suffering from sudden onset of dizziness. A giant right middle cerebral artery dissecting aneurysm was found.
• Past medical history: No HTN OR DM. Neither smoking or drinking.
• Medication:-.
• NE: (-).
• 68岁 男性。
• 突发头晕,检查发现右侧大脑中动脉巨大夹层动脉瘤。
• 既往史:否认高血压、糖尿病,否认吸烟饮酒。
• 药物:-。
• 神经查体:-。



图 4. 3D重建提示右侧大脑中不规则夹层动脉瘤,动脉瘤累及M1主干。
1
Strategy
• The giant lobular M1 segment dissecting aneurysm with a high risk of bleeding or occlusion should be treated.
• Conventional technique-conventional stent assisted large coil was economical but harbored a relative high recurrence risk.
• Pipeline was another choice for this kind of aneurysms, with a low recurrence risk but delayed rupture or occlusion risks.
• Staged operation-first stage for simple coil embolization and second stage for Pipeline deployment will be adopted in order to reduce a delayed bleeding risk.
• The distal aneurysm sac possessed a high rupture risk, which will be embolized at the first stage.
• Dual antiplatelet therapy will be administered after the first stage.
• 大脑中M1段巨大分叶状夹层动脉瘤,出血或血管闭塞风险高,建议治疗。
• 传统的方法——普通支架辅助大圈栓塞更经济,但相对复发风险高。
• 这类夹层动脉瘤也可以选择Pipeline,复发风险低,但有延迟出血或血管闭塞风险。
• 为了降低复发和延迟破裂风险,我们采用分期治疗,一期单纯栓塞,二期Pipeline支架置入。
• 该动脉瘤远端瘤腔破裂风险高,一期弹簧圈栓塞降低出血风险。
• 一期治疗后予双抗口服。
2
Stage 1. Simple coiling



图 10. 3D重建显示弹簧圈成篮。
3
Post Operation
• NE: GCS 15, no headache or dizziness, normal bilateral muscle strength.
• Medication: Tirofiban 7ml/h maintained for 24 hours. Clopidogrel and Aspirin.
• 神经查体:GCS 15,无头痛头晕,四肢肌力正常。
• 药物:替罗非班7ml/h微泵维持24h。口服氯吡格雷及阿司匹林。
4
Pipeline deployment (5d after 1st stage)
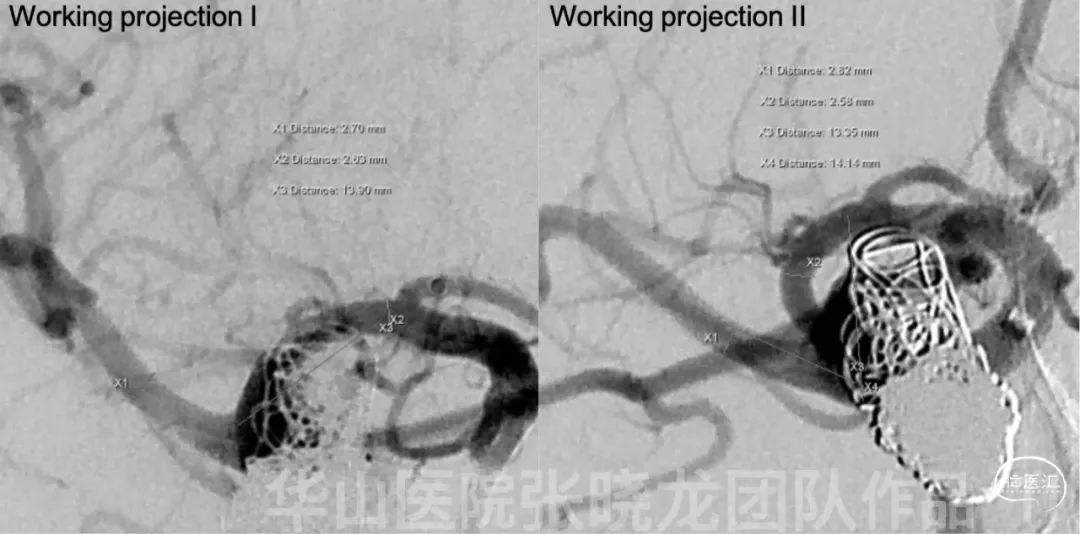
Figure 11. Choose two different working projections. Measurements: proximal parent artery diameter 2.5mm and distal parent artery diameter 2.8mm.

Figure 13 GIF. Deploy Pipeline 3mm*20mm stent from M2 to M1 segment covering the aneurysm neck.

Figure 15 GIF. Angiography showed the aneurysm sac almost non-visualization. Rational DSA depicted the stent well-opened and well-adherence.
图 16 GIF. 载瘤动脉动脉通畅,颅内未见出血及血栓。
5
Post-operation
• NE: GCS 15, no headache or dizziness, normal bilateral muscle strength, bilateral Babinski negative, no new neurological deficit.
• Medication: Clopidogrel and Aspirin ( ADP 97%, AA 100%).
• At discharge: Clopidogrel for three months and Aspirin for long-term.
• 神经查体:GCS 15,无头痛头晕,四肢肌力正常,双侧巴氏征阴性,无新发神经功能缺损。
• 术后用药:口服氯吡格雷和阿司匹林(氯吡格雷抑制率97%,阿司匹林抑制率100%)。
• 出院:氯吡格雷口服3个月,阿司匹林长期口服。
6
13 month follow up

Video 1. Rational DSA showed the right middle cerebral artery inferior trunk became slender by the follow-up.
Video 2. The intra-stent was a severe stenosis by 3 month follow up while the stenosis improved by 13 month follow up.
Video 3. The parent artery was patent by follow up.

图 18. 3个月MRA随访示动脉瘤腔仍有显影,支架近端明显狭窄;13个月随访动脉瘤不显影,支架内狭窄好转。
7. Summary
1. The giant lobular M1 segment dissecting aneurysm with a high risk of bleeding or occlusion should be treated.
2. Conventional technique-conventional stent assisted large coil was economical but harbored a relative high recurrence risk.
3. Pipeline was another choice for this kind of aneurysms, with a low recurrence risk but delayed rupture or occlusion risks.
4. Staged operation-first stage for simple coil embolization and second stage for Pipeline deployment was adopted in order to reduce a delayed bleeding risk.
5. The distal aneurysm sac possessed a high rupture risk, which was embolized at the first stage.
6. Tirofiban maintained for 24 hours after simple coiling because of the wide-necked dissecting aneurysm and protecting against thrombus formation.
7. Dual antiplatelet therapy was administered after the first stage.
8. Multiple working projections to deploy and observe the Pipeline for full-open and well-adherence.
9. Intra-stent severe stenosis was observed by 3 month follow-up and LDL was 2.77mmol/L. Therefore, Atorvastatin was prescribed. The stenosis improved when 13 month follow-up (LDL 1.41 mmol/L).
10. Continue statin and Clopidogrel for long-term and next follow up was scheduled in 2-3 years.
1. 大脑中M1段巨大分叶状夹层动脉瘤,出血或血管闭塞风险高,建议治疗。
2. 传统的方法——普通支架辅助大圈栓塞更经济,但相对复发风险高。
3. 这类夹层动脉瘤也可以选择Pipeline,复发风险低,但有延迟出血或血管闭塞风险。
4. 为了降低复发和延迟破裂风险,我们采用分期治疗,一期单纯栓塞,二期Pipeline支架置入。
5. 该动脉瘤远端瘤腔破裂风险高,一期弹簧圈栓塞降低出血风险。
6. 由于该夹层动脉瘤宽颈,为防止弹簧圈形成血栓后逃逸栓塞血管,一期单纯栓塞术后予替罗非班7ml/h维持24h。
7. 一期治疗后予双抗口服。
8. 二期pipeline支架释放选用多个工作角度观察释放,支架完全打开贴壁。
9. 3个月随访时支架内严重再狭窄,低密度脂蛋白2.77mmol/L,予口服阿托伐他汀。13个月随访时支架内再狭窄消失,患者低密度脂蛋白1.41mmol/L。
10.建议继续口服阿司匹林及氯吡格雷,2-3年后随访。
8
Reference
1 张学贤,杨凯,冯超凡,万程,赵卫,胡继红,孟雪柔,李自恒.颅内动脉瘤支架植入术后新生内膜增生临床研究[J].介入放射学杂志,2022,31(04):328-332.

张晓龙
复旦大学附属华山医院
复旦大学附属华山医院放射科主任医师,博士、教授、博士生导师;
斯坦福大学医学院客座临床教授;
主持国家自然科学基金3项,第一作者或通讯作者发表国内外权威期刊文章50余篇;
中华医学会、放射学会、卫生部医政司等组织中担任副主任委员、组长等职务.《中国名医百强榜》神经介入专业中国十强(2012年度、2013年度、2014年度、2015-16年度、2017-18年度);
擅长复杂和疑难脑血管疾病的介入治疗,如复杂脑动脉瘤的栓塞,硬脑膜动静脉瘘栓塞,脑动静脉畸形栓塞,脑梗死的支架,脊髓血管畸形治疗;
自1995年开始从事脑血管疾病介入诊治工作和研究,师从黄祥龙教授、沈天真教授和凌锋教授,是我国最早从事神经介入的专家之一。2010年9月至今连续介入治疗颅内动脉瘤1500余例,无操作致死。
.png")
点击或扫描上方二维码,
前往 张晓龙教授 学术主页
查看更多精彩内容

点击或扫描上方二维码
查看更多“介入”内容
