


Case Review
• 66 y/o, male.
• suffered from paroxysmal dizziness, slurred speech accompanied with right limb weakness (V-) 6 months, with the sequela of right hand inflexibility. Though antiplatelets were taken, recurrent TIA remained.
• EMG shows possible nerve damage. Local hospital MRI confirmed left parietal infarctions. CTA visualized Left M2 segment severe stenosis.
• Past medical history: HTN for 15 years, well-controlled. No DM or alcohol consumption, smoking for 30 years and quitting for 4 months. History of gastric bleeding and fecal occult blood positive, so Aspirin was ceased.
• Medication: Cilostazol, Clopidogrel, Atorvastatin, Felodipine Sustained-Release Tablets, Tamsulosin Sustained-Release Capsules, Finasteride.
• NE: inflexible right hand.
• 66岁,男性。
• 主诉:发作性头晕、言语不清伴右侧肢体无力(V-)6月,遗留右手不灵活。尽管口服双抗,仍有反复发作性TIA。
• 外院肌电图提示神经损伤可能。当地医院头颅MRI提示左侧顶叶脑梗死,CTA提示左侧大脑中M2段重度狭窄。
• 既往史:高血压15年,平素血压控制好;否认糖尿病及饮酒史,吸烟30年戒烟4月。胃出血病史,服用阿司匹林后血便隐血阳性,故停用阿司匹林。
• 药物:西洛他唑,氯吡格雷,非洛地平缓释片,坦索罗辛缓释片,非那雄胺。
• 神经查体:右手不灵活。

图 1. DWI提示左侧顶叶急性脑梗死。

图 2. CTA提示左侧大脑中动脉M2段重度狭窄,狭窄处未见明显钙化。

图 3 GIF. SWI未见明显微出血。

图 4 GIF. 高分辨MRI提示左侧大脑中动脉狭窄段管壁明显强化。

图 5. CTP未见明显低灌注。

图 6. 双侧椎动脉及基底动脉未见狭窄。

图 7. 左侧颈内动脉颈段及右侧颈内动脉未见明显狭窄。

图 8 GIF. 造影证实左侧大脑中动脉M2段重度狭窄。
1
Strategy
Indications: Although no obvious hypoperfusion was detected on CTP, recurrent TIA remained in administration of antiplatelets. The negative results of CTP postulated as following reasons: inaccurate results of CTP or repeated focal thrombosis formation then resolution leading to repeated TIA.
Medical images confirmed the left M2 segment severe stenosis with a large angle on the large diameter middle trunk.
Neuroform stenting was preferred instead of Wingspan to avoid stent kinking or malposition.
Postoperative blood pressure should be monitored to prevent hyper-perfusion.
治疗指针:尽管CTP没有明显低灌注,但在口服双抗的情况下仍有TIA发作。CTP阴性结果考虑原因:可能是CTP不准确或是反复局部血栓形成、再通,导致TIA反复发作。
影像学证实左侧大脑中动脉M2段中干重度狭窄,中干粗大,且成角大。
为避免支架折弯或移位,首选Neuroform支架而不是Wingspan支架。
为防止高灌术后应严格控制血压。
2
Operation
图 9 GIF. 测量:狭窄近端血管直径2.82mm、远端2.38mm。将6F Envoy DA导引导管置于左侧颈内动脉海绵窦段,将Gateway 2.25*15mm在Floppy 300交换导丝导引下置于左侧大脑中动脉狭窄段。以6ATM充盈球囊10s,复查造影未见出血,狭窄段扩张满意。撤出球囊,行全身肝素化。
图 10 GIF. 将XT-27在Floppy交换导丝导引下置于大脑中动脉M2段远端,于狭窄处释放Neuroform 2.5*15mm支架,支架中段扩张欠满意。

图 11 GIF. Gateway 2.5*9mm球囊在Floppy-300导丝(头端塑J型)导引下置于狭窄段,以4ATM充盈球囊扩张15s,手推造影无出血。再次以3ATM充盈球囊15s,卸除球囊后手推造影证实无出血。
图 12. 复查造影证实狭窄段扩张满意。
Figure 13 GIF. The intracranial vessels were intact.
图 13 GIF. 颅内血管完好。
图 14. Dyna-CT未见出血。
3
Post Operation
Medication: Keep systolic pressure between 100-130mmHg. Tirofiban 4ml/h maintained for 24h. Cilostazol and Ticagrelor were prescribed ( TEG ADP 5.9%) .
NE: GCS 15, fluent speech, normal muscle strength, no new neurologic defect.
At discharge: Ticagrelor for 6 month and Cilostazol plus Atorvastatin for long-term.
药物:严格控制收缩压,收缩压维持在100-130mmHg。替罗非班4ml/h微泵维持24h。口服西洛他唑和替格瑞洛(血栓弹力图:氯吡格雷抑制率5.9%)。
查体:GCS 15,言语清,四肢肌力正常,无新发神经功能缺损症状。
出院:替格瑞洛口服6月后停药,西洛他唑和阿托伐他汀长期口服。
4
Follow Up
No TIA or infarction was occurred after operation.
Blood pressure and blood lipid (LDL 1.26 mmol/L) controlled well. No DM or drinking or smoking.
Cilostazol and Atorvastatin were taken regularly.
术后患者无TIA或脑梗发作。
患者血压及血脂控制良好(低密度脂蛋白 1.26mmol/L),无糖尿病,不吸烟,不饮酒。
长期规律口服西洛他唑和阿托伐他汀。
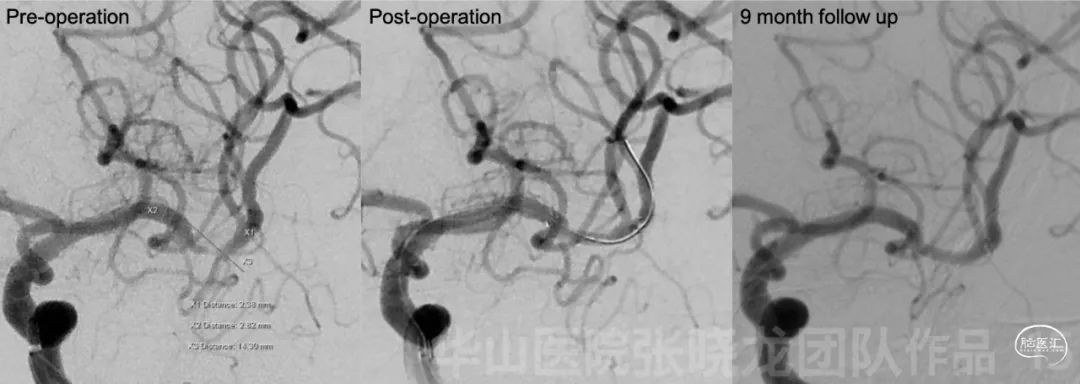
图 15. 9个月随访支架内无再狭窄。
Video 1. Rotational DSA displayed the artery was patent without stenosis.
视频 1. 旋转DSA证实血管通畅,支架内无再狭窄。
Video 2. The intracranial vessels were intact.
Summary
Although no obvious hypoperfusion was detected on CTP, recurrent TIA remained in administration of antiplatelets.
The negative results of CTP postulated as following reasons: inaccurate results of CTP or repeated focal thrombosis formation then resolution leading to repeated TIA.
Left M2 segment stenosis with a large angle was located at the large diameter trunk.
Relative large balloon dilation could be adopted because the stenosis locating at the large diameter trunk and no obvious perforators originating from the stenosis. If the stenosis located at the small diameter trunk (<2mm), simple balloon dilation or drug coated balloon was selected.
Neuroform stent was preferred instead of Wingspan to avoid stent kinking or malposition.
Postoperative systolic pressure should be monitored to prevent hyper-perfusion. Next follow up was scheduled in 3 years.
Post-dilation could be performed for insufficient stent expansion.
Good management of risk factors such as smoking, blood sugar and blood lipid contribute to a good prognosis.
Continue Cilostazol and Atorvastatin for long-term. Next CTA follow up was scheduled in 2 years.
尽管CTP没有明显低灌注,但在口服双抗的情况下仍有TIA发作。
CTP阴性结果考虑原因:可能是CTP不准确或是反复局部血栓形成、再通,导致TIA反复发作。
左侧大脑中动脉M2段中干重度狭窄,中干粗大,且成角大。
该病例狭窄段血管较粗大,且未见明显穿支发出,可以选用相对大的球囊扩张;若狭窄段血管较细(<2mm),可以选择单纯球囊扩张或药物球囊扩张。
为避免支架折弯或移位,首选Neuroform支架而不是Wingspan支架。
为防止高灌术后应严格控制血压。
支架打开不良,采用球囊后扩。
术后危险因素(如吸烟、高血糖、高血脂)的控制十分重要。
长期口服西洛他唑及阿托伐他汀,2年后门诊复查头颅CTA。

张晓龙
复旦大学附属华山医院
复旦大学附属华山医院放射科主任医师,博士、教授、博士生导师;
斯坦福大学医学院客座临床教授;
主持国家自然科学基金3项,第一作者或通讯作者发表国内外权威期刊文章50余篇;
中华医学会、放射学会、卫生部医政司等组织中担任副主任委员、组长等职务.《中国名医百强榜》神经介入专业中国十强(2012年度、2013年度、2014年度、2015-16年度、2017-18年度);
擅长复杂和疑难脑血管疾病的介入治疗,如复杂脑动脉瘤的栓塞,硬脑膜动静脉瘘栓塞,脑动静脉畸形栓塞,脑梗死的支架,脊髓血管畸形治疗;
自1995年开始从事脑血管疾病介入诊治工作和研究,师从黄祥龙教授、沈天真教授和凌锋教授,是我国最早从事神经介入的专家之一。2010年9月至今连续介入治疗颅内动脉瘤1500余例,无操作致死.
.png")
点击或扫描上方二维码,
前往 张晓龙教授 学术主页
查看更多精彩内容

点击或扫描上方二维码
查看更多“介入”内容
