


Case Review
History
• 53 y/o, male
• 神经查体:(-)。
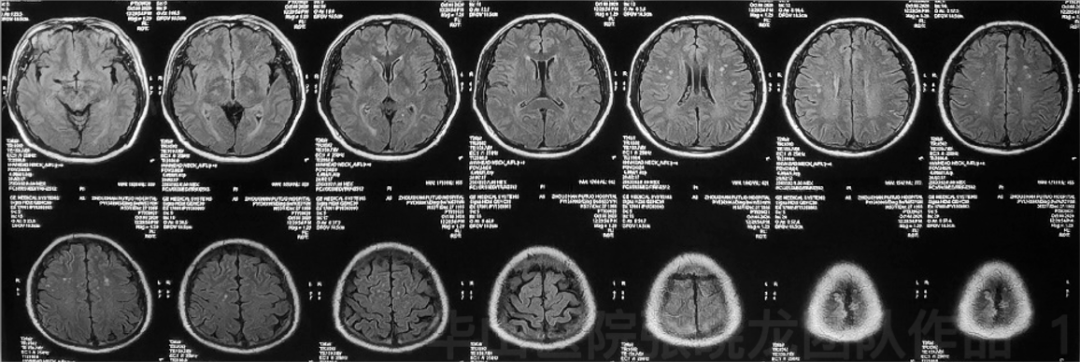
Figure 1. T2 Flair shows scattered small infarctions. T2 Flair显示散在小梗死灶。
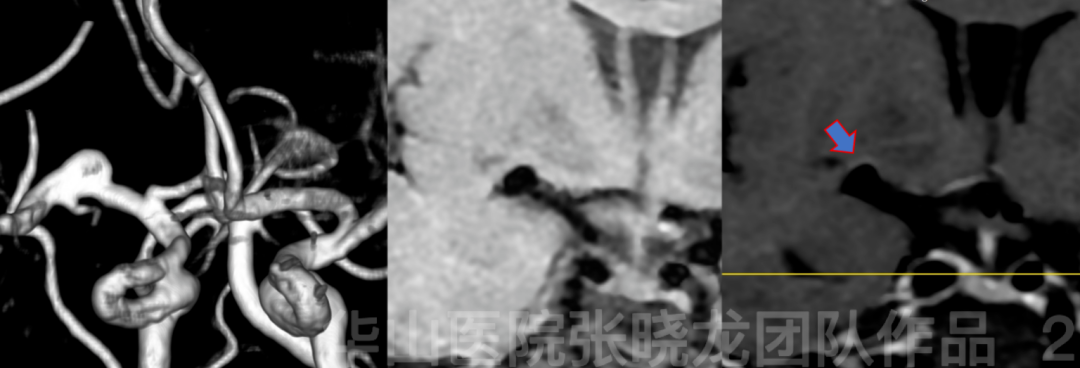
Figure 2. Multi-model MRI shows a right M1 dissecting aneurysm with partial enhanced aneurysmal wall. 多模态MRI显示右侧大脑中动脉M1段夹层动脉瘤,部分瘤壁强化。
Video 1. Angiography confirms a right MCA dissecting aneurysm incorporating lenticular arteries (red arrow). 血管造影证实右侧大脑中动脉夹层动脉瘤累及豆纹动脉(红色箭头)。
1
Strategy
SAC (Stent-assisted coiling)-Decrease recurrence rate
2
Operation
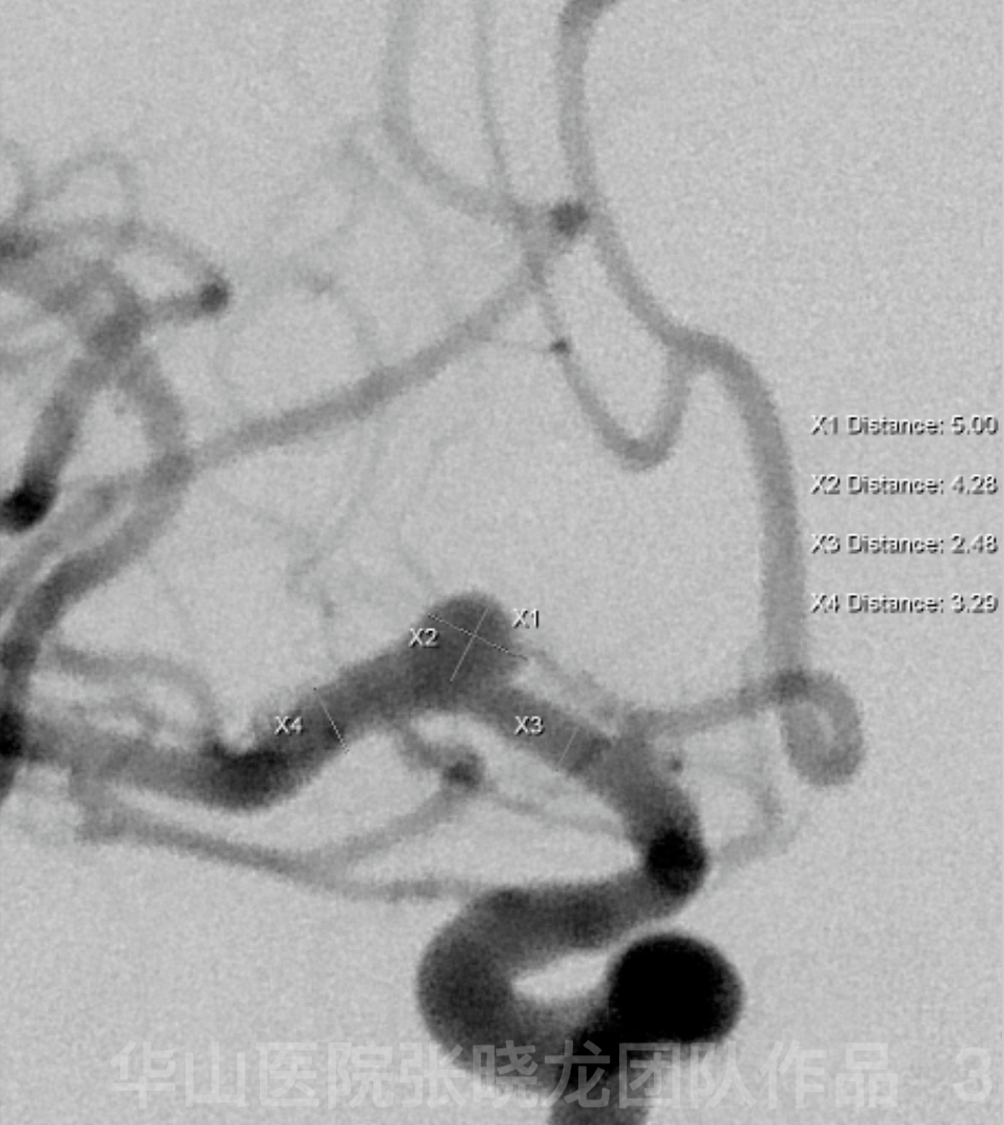
Figure 3. Measurement. 测量。
Video 2. General heparinization.6F guiding catheter. A Prowler plus microcatheter was advanced to the M2 branch guided by a Synchro-2 microwire. An Echelon-10 microcatheter with a straight tip was navigated to the aneurysmal sac. Microplex-10 4mm*10cm coil was selected for framing which was unsatisfactory. 全身肝素化。6F导引导管。在Synchro-2微导丝引导下,将一根Prowler plus微导管推送到M2段分叉处。Echelon-10直头微导管到达动脉瘤腔。选用Microplex-10 4mm*10cm弹簧圈成篮,但结果不理想。
Video 3. A Solitaire 4*20mm stent was deployed via the Prowler Plus microcatheter. 通过Prowler Plus微导管置入一枚Solitaire 4*20mm支架。
Figure 4 GIF. A successful coil framing was made by the Microplex-10 4mm*10cm after stent deployment. At the same time, the tip of the coiling microcatheter was pushed out of the aneurysmal sac. 支架释放后,使用Microplex-10 4mm*10cm弹簧圈顺利成篮。同时,栓塞微导管头端已脱出瘤腔。

Figure 5 GIF. The tip of the coiling microcatheter was renavigated to the aneurysmal sac guided by a microwire. 栓塞微导管的头端在微导丝引导下重新到达动脉瘤腔内。
Figure 6 GIF. Six coils were inserted into the aneurysmal sac. Hypersoft 3mm*8cm (1), Hypersoft 1.5mm*4cm (2), Hypersoft 2mm*3cm (1) ,Target 360 2mm*3cm (1), Target 360 2mm*4cm (1). But post-coiling angiography shows thrombosis in the parent artery and suspected hemorrhage. 6枚弹簧圈被填入动脉瘤腔:Hypersoft 3mm*8cm一枚,Hypersoft 1.5mm*4cm两枚, Hypersoft 2mm*3cm一枚,Target 360 2mm*3cm一枚,Target 360 2mm*4cm一枚。但是,栓塞后血管造影可见载瘤动脉血栓形成和可疑出血。
Figure 7 GIF. Repeated angiography shows no hemorrhage. 复查血管造影未见出血。
Figure 8 GIF. Dyna CT also confirms no hemorrhage. Dyna CT也证实没有出血。

Figure 9 GIF. After given Tirofiban 16ml and Nimodipine 1ml via the guiding catheter, the angiography shows complete dissolution of the thrombus and patent lenticular arteries arising from the neck region of the aneurysm. 经导引导管给予替罗非班16ml和尼莫地平1ml后,血管造影显示血栓完全溶解,动脉瘤颈发出的豆纹动脉通畅。
3
Post-operation
• No neurologic deficit.
• Medications: Clopidogrel 75mg qd for three months, Aspirin 100mg qd until next follow up, anti-hypertensive medicine.
4
Follow up

Figure 10 GIF. Seven-month follow up angiography shows densely packing of the aneurysm with parent artery patent. 7个月随访血管造影显示动脉瘤致密栓塞,载瘤动脉血流通畅。
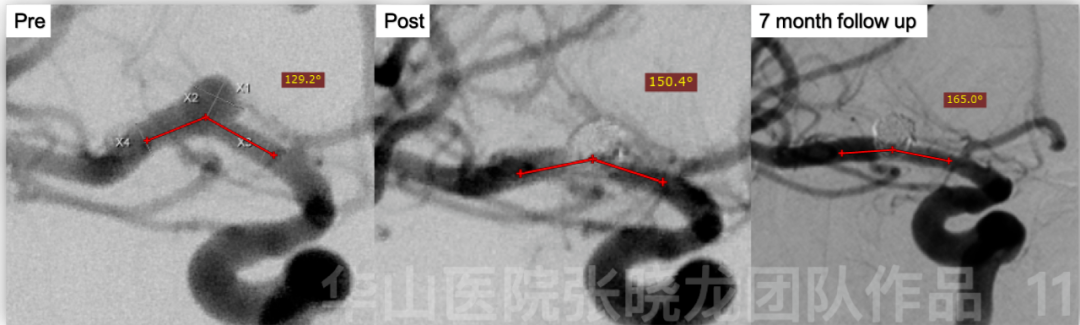
Figure 11. Compared with span and post treatment angiography, follow up angiography shows the parent artery angle increases from 129.2 degrees to 165.0 degrees. 与治疗前后血管造影相比,随访血管造影显示载瘤动脉角度由129.2°进一步增加到165.0°。
4
Summary
• Indications: aneurysm wall enhancement and ischemic symptoms

