


Our case
History
• 既往史:高血压病史11年;否认糖尿病史;吸烟史45年余。患者既往右侧中枢性面瘫三次(2009年、2011年、2013年),胃出血两次。
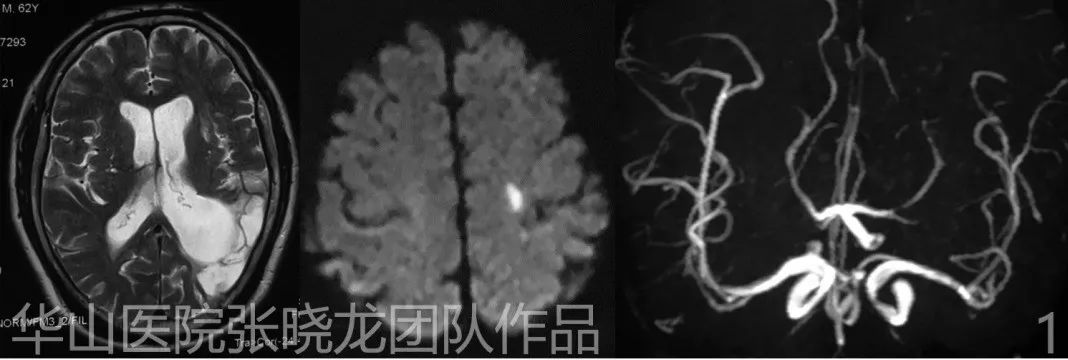
Figure 1. Acute infarction on left spancentral gyrus. Chronic infarction on left temporal lobe. Right PcomA AN. 左侧中央前回急性梗塞灶;左侧颞叶慢性梗塞灶;右侧后交通动脉瘤。
1
Strategy
2
Operation
Video 3. Dual microcatheter plus stent assisted technique was chosen to densely pack the main sac while only loosely packing the daughter sac. Therefore the microcatheter should not be inserted deeply into the daughter sac. The initial coil (MicroPlex 3mm*8cm) entered the daughter sac spansenting a rupture risk. 采用双微导管加支架辅助技术致密栓塞动脉瘤主囊,而子囊仅疏松栓塞。因此,微导管不应深入子瘤内。首枚填入子囊内的MicroPlex 3mm*8cm弹簧圈存在破裂风险。
Figure 2 GIF. Insert the second coil (Microplex 2mm*8cm). The microcatheter was readjusted to retrieve the coil and placed it in the main sac, although the microcatheter was quite unstable. 填入第二枚Microplex 2mm*8cm弹簧圈。微导管较为不稳定,重新调整微导管以回收弹簧圈并重新填入动脉瘤主囊内。
Figure 3 GIF. For a better vision of the neck of aneurysm and deployment of the stent,we changed working projection. Then one Neuroform 4mm*20cm was advanced across the protruded loop. 我们更换支架释放工作角度。然后可见Neuroform 4mm*20cm支架通过之前脱出的襻环。
Figure 4 GIF. As coils protruded into the parent artery, one microcatheter was retrieved to free space in the sac. 当弹簧圈突入载瘤动脉时,回撤一根微导管以空出瘤腔内的空间。
Figure 5 GIF. Neuroform is easy to rebound. So the stent was deployed from the origin of MCA. General heparinization. Neuroform支架容易弹回,所以从大脑中动脉起始部开始释放支架。行全身肝素化。

Figure 6 GIF. MicroPlex 2mm*6cm.

Figure 7 GIF. Microplex 2mm*3cm,four coils in all. Microplex 2mm*3cm,共四枚弹簧圈。

Figure 8 GIF. The way of retrieving the microcatheter after coiling. 弹簧圈栓塞后微导管的回收方法。
Figure 9 GIF. Post-operative angiography shows densely packing of the aneurysm and the contrast media stagnation in the daughter sac. 术后血管造影显示动脉瘤致密栓塞,子瘤内有造影剂滞留。
Figure 10 GIF. Intracranial vessels are intact and the parent artery is patent. Tirofiban (Xinweining) 20ml was given via the guiding catheter. 颅内血管显示完整,载瘤动脉通畅。经导引导管给予替罗非班(欣维宁)20ml。
3
Post operation
• No more neurologic deficit.
Figure 11 GIF. 4 year follow up angiography shows no relapse of the aneurysm. 4年随访血管造影未见动脉瘤复发。

Figure 12. The aneurysm was densely packed without relapse in 4 year follow up angiography. The shape of coils kept stable. 4年随访,血管造影显示:动脉瘤致密栓塞,未见复发。弹簧圈形态保持稳定。

Figure 13. Comparison of coils and stent between post-operation, 7 month follow up and 4 year follow up. 术后即刻、7个月随访和4年随访,弹簧圈和支架的比较。
4
Summary
![]()
