

对于每一位神经外科医师来说,翼点入路(pterional approach)大概都是启蒙级入路吧。然而,除了翼点的定义(图0)和罗列的一条条手术适应症和手术步骤外,对于这个几乎万能的幕上入路的“前世今生”,各大教科书似乎都很少涉及。个人觉得,对一个入路的学习,应该包括其发展和演变;了解它的历史,才能更好地掌握现状和构想未来。今天,就来简单罗列一下翼点入路的编年史。
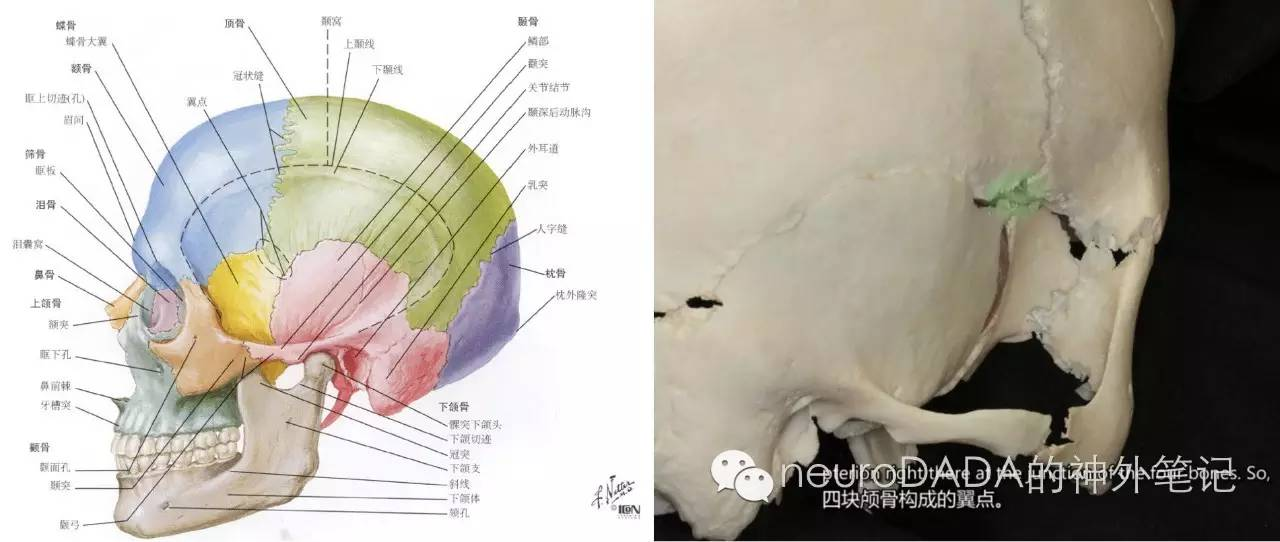
图0
Durante,1885:sub/transfrontal,嗅沟脑膜瘤,1st额下入路
Horsley,1889:frontal,垂体瘤,失败,1st暴露垂体
Krause,1900:1stextradural supraorbital subfrontal,视神经部位取子弹,1ststrict frontal变为lateral frontal
Krause,1905-1909:frontolateral,鞍区肿瘤,类似当今(图1-上左)
McArthur,1908:frontal intradural,失败;
McArthur,1912:frontal extradural+superior orbital roof/rim=1stcranioorbital craniotomy,眶颧入路的鼻祖
Frazier,1913:从transsphenoidal回到subfrontal处理垂体瘤,类似McArthur,extradural cranioorbital craniotomy(图1-上右)
Cushing,1916:subfrontal,1st全切鞍结节脑膜瘤(图1-下)
Frazier,1919:intradural frontal(lateral)
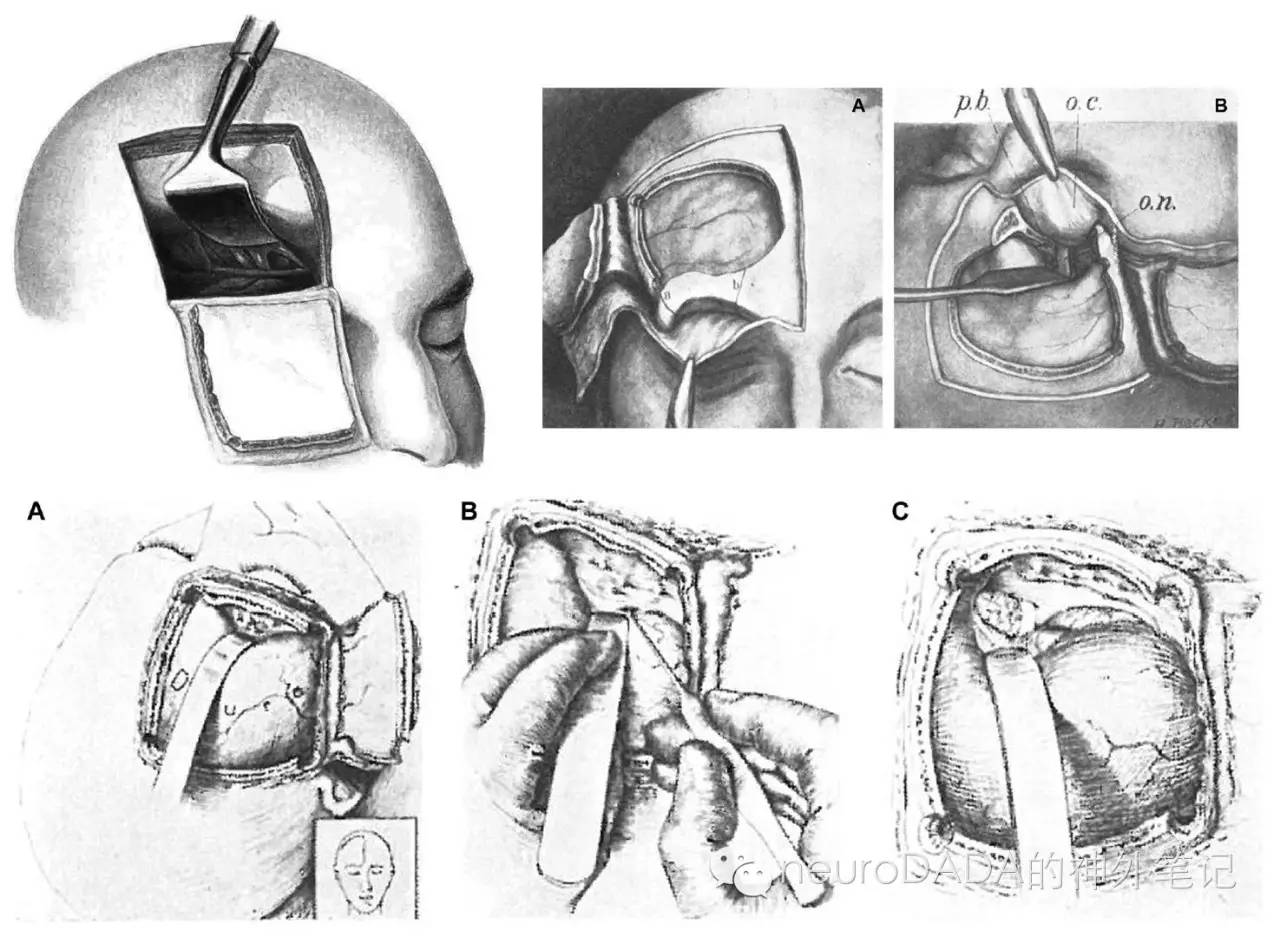
图1
Heuer,1914:1stintradural frontotemporal,视交叉病变,当今翼点入路鼻祖,类似于Krause的intradural frontolateral,区别在于骨瓣包含temporal bone(图2-1)
Dandy,1918:报道上者,(图2-2)
Dandy,1922:经额颞入路经终板三脑室造瘘,梗阻性脑积水,需断视神经
Dandy,1932:改进,小切口——Dandy flap,hypophyseal approach,鞍区病变,(图2-3)
Dandy,1937:1st前循环动脉瘤(图2-4)
Hayes,1962:小号的Dandy flap,ACom动脉瘤
Rizzoli,1953:前循环动脉瘤
Hamby,1964:1st起名pterional approach,眼眶肿瘤、突眼症(图3-A)
Kempe,1968-1971:ACom动脉瘤,1st定义关键孔psychopathic point(图3-B)
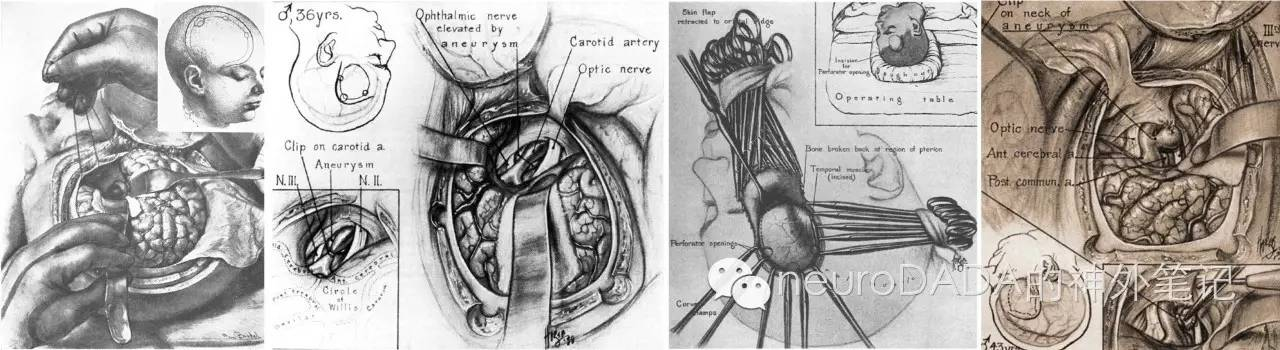
图2
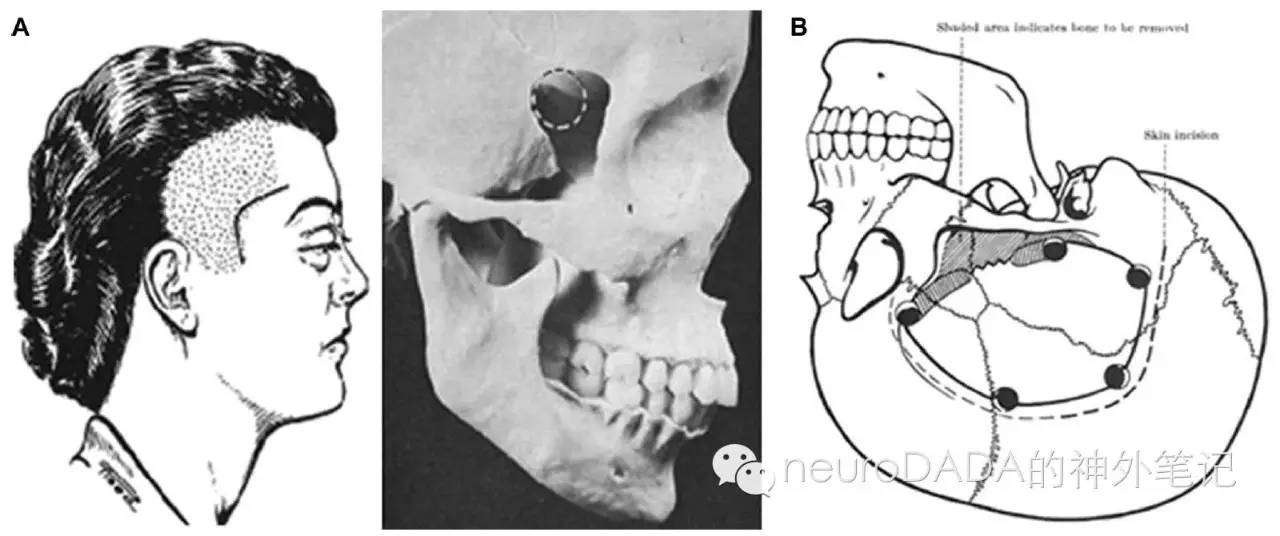
图3
Falconer,1951:unilateral frontal craniotomy,分离侧裂,ICA分叉部、ACom、MCA动脉瘤(图4-上左)
Poppen,1951:unilateral frontal craniotomy,ACom动脉瘤(图4-上右)
Norlen & Barnum,1953:unilateral frontal craniotomy,ACom动脉瘤(图4-下左)
Hamby,1952,1954:unilateral frontal craniotomy,前循环动脉瘤(MCA除外)(图4-下右A);frontotemporal craniotomy,分离侧裂,MCA动脉瘤(图4-下右B)
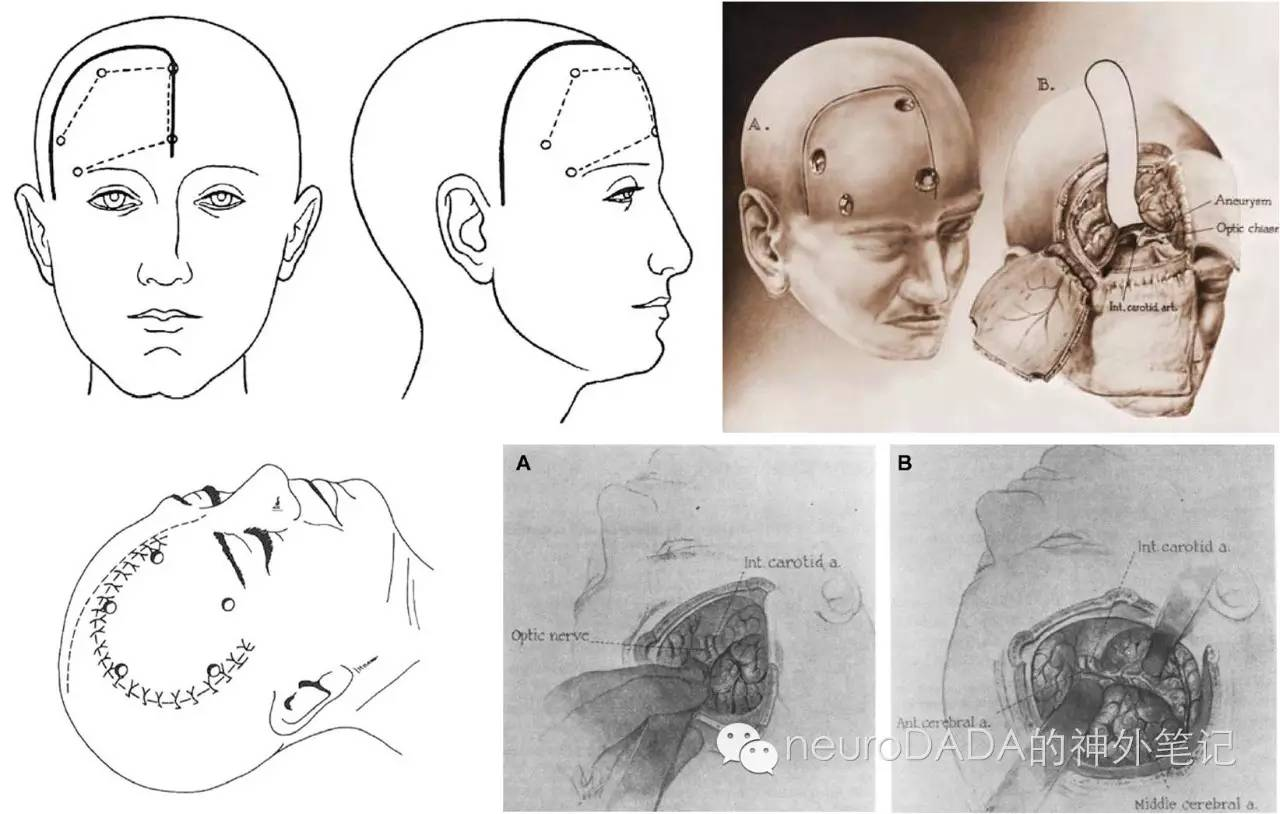
图4
House,1961:1st显微外科,听神经瘤
Yasargil,1969:显微神经外科之父,显微器械,cisternal approach,引入keyhole锁孔概念,翼点开颅规范化,仍然采用psychopathic point作为关键孔,另加3个孔,硬膜外磨除蝶骨翼(key landmark),frontolateral、spheno-orbital、pterional approach,区别先人——小切口、小骨窗、更基底,从而扩展至基底动脉顶端动脉瘤的夹闭(图5)

图5
1、联合颞下处理后循环动脉瘤
Drake,1978:“half and half”—— pterional+subtemporal,后循环动脉瘤,侧方观察穿支
Sano,1980:temporopolar,基底动脉尖动脉瘤
Shiokawa,1989:zygomatic temporopolar,高位基底动脉尖动脉瘤
Heros & Lee,1993:pterional+anterior temporal,后循环动脉瘤,侧方观察穿支
de Oliveira,1995:pretemporal approach,脚间池、岩斜区(图6)

图6
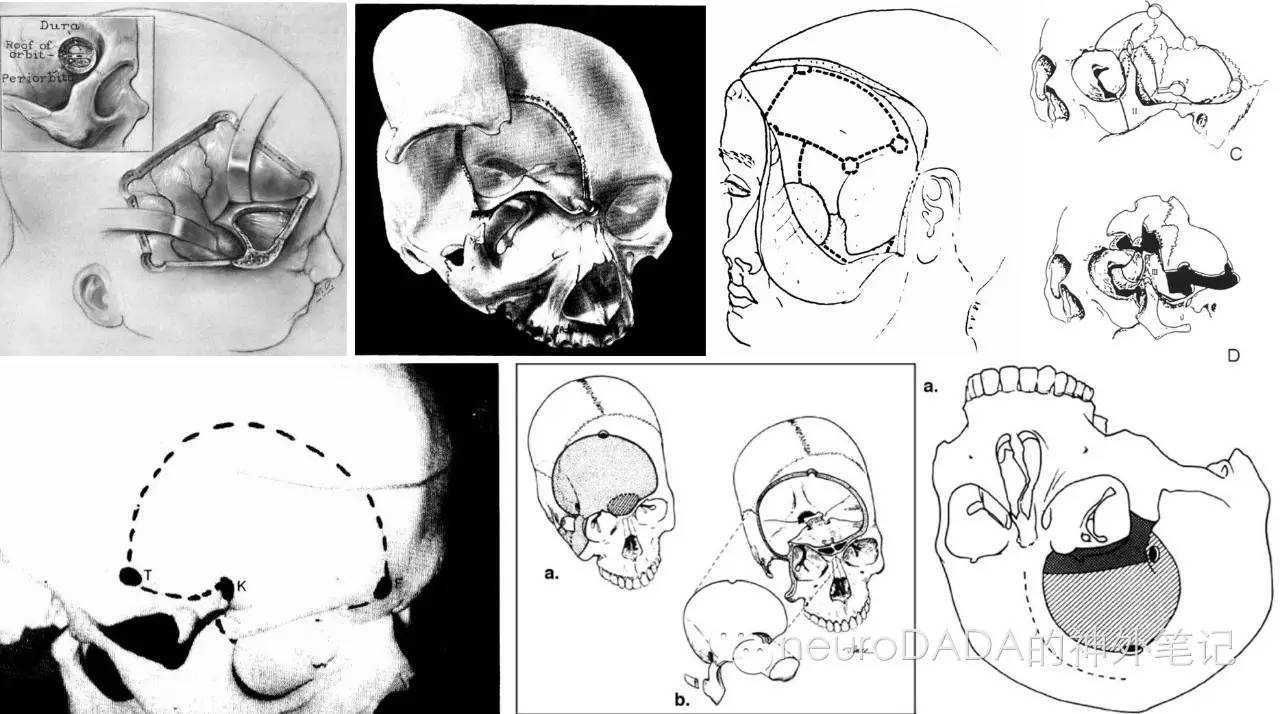
图7
2、额颞眶颧入路
MacCarty,1961:frontal craniotomies,1st单孔处理眶内病变,MacCarty burr hole(图7-上1)
Jane,1982:supraorbital-frontal approach,1-piece,鞍区、眶内病变、动脉瘤(图7-上2)
Pellerin,1984:orbitofrontomalar,1st+去颧弓,2-piece,额颞蝶脑膜瘤(图7-上3)
Hakuba,1986,1989:orbitozygomatic infratemporal (3 complicated muscle-based bone flaps),高位基底动脉尖动脉瘤、海绵窦肿瘤、三脑室肿瘤(图7-上4)
Al-Mefty,1987:Supraorbital-pterional approach,1-piece,颅底病变(图7-下左)
Alaywan & Sindou,1990:Fronto-temporal approach withorbitozygomatic removal(FTOZ),2-piece
Delashaw (Rhoton),1992:modified supraorbital approach (2 step: frontotemporal+frontal sinus+superior/lateralorbital ridges,zygomatic arch)(图7-下中)
Delfini,1992:two-step supraorbital approach
Sekhar,1994:FTOZ,2-piece(图7-下右)
Zabramsky (Spetzler),1998:FTOZ,2-piece(图8-左)
Aziz,2002:FTOZ,1-piece(图8-中)
Campero ( Rhoton),2010:FTOZ,3-piece(图8-右)

图8
3、硬膜外前床突切除术——Dolenc入路处理海绵窦病变(图9)
Dolenc,1985:combined epi- and subdural direct approach,眼动脉瘤
Dolenc,1987:transcavernous-transsellar,基底动脉尖动脉瘤
Dolenc,1994:Frontotemporal epidural approach,三叉神经鞘瘤
Dolenc,1997:Transcranial epiduralapproach,侵袭性垂体瘤
Dolenc,1999:Extradural approach,海绵窦段动脉瘤
Dolenc,1999:combined transorbital-transclinoid andtranssylvian approach,眼动脉瘤

图9
4、局限化的眶上入路
Brock & Dietz,1978:更小的皮瓣,动脉瘤,有图(图10)
van Lindert,1998:supraorbital keyhole,动脉瘤
Czirjak,2001:trans-supraorbital
Ramos-Zuniga,2002:trans-supraorbital
Steiger,2001:orbitocranial,ACom动脉瘤
Reisch,2002,2005:eyebrow skin incision supraorbital(图11)
Hernesniemi,2005:Lateral supraorbital approach(图12)
Figueiredo,2006:mini-supraorbital
Figueiredo,2007:minipterional
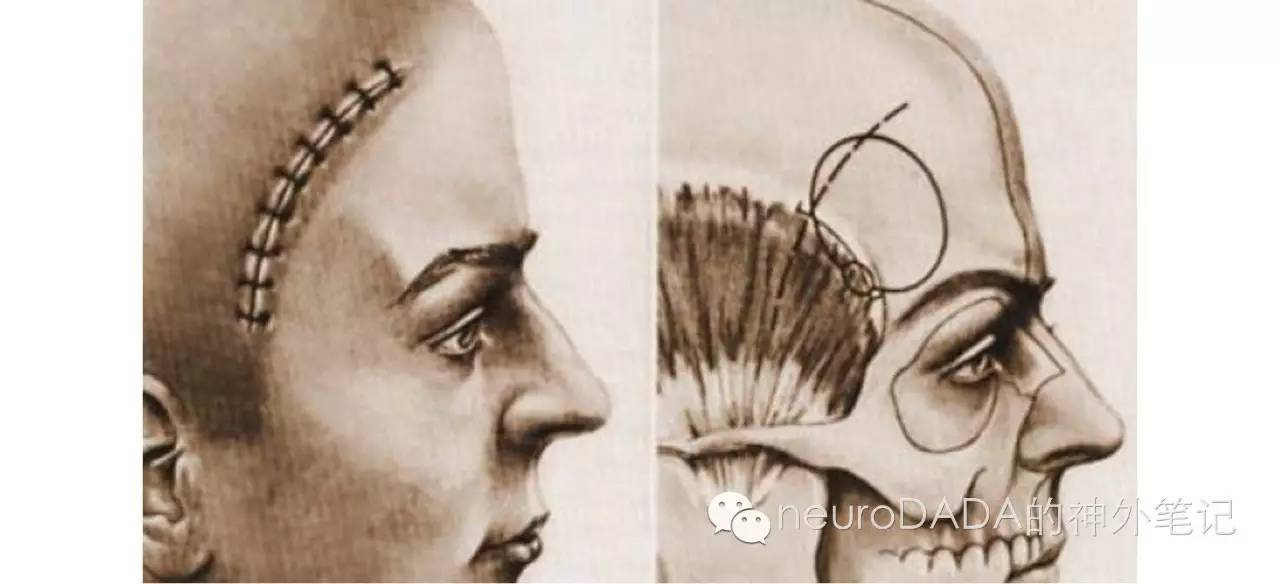
图10
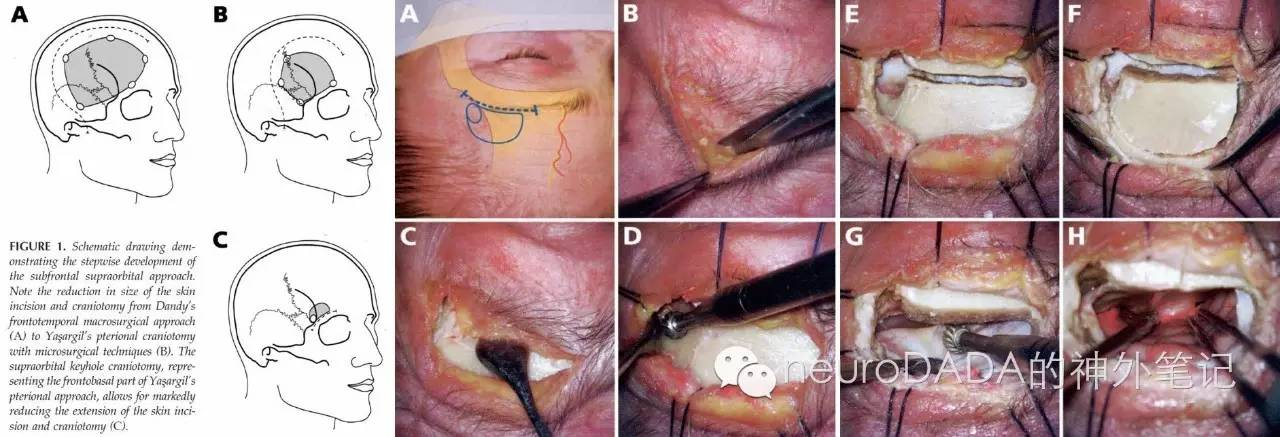
图11
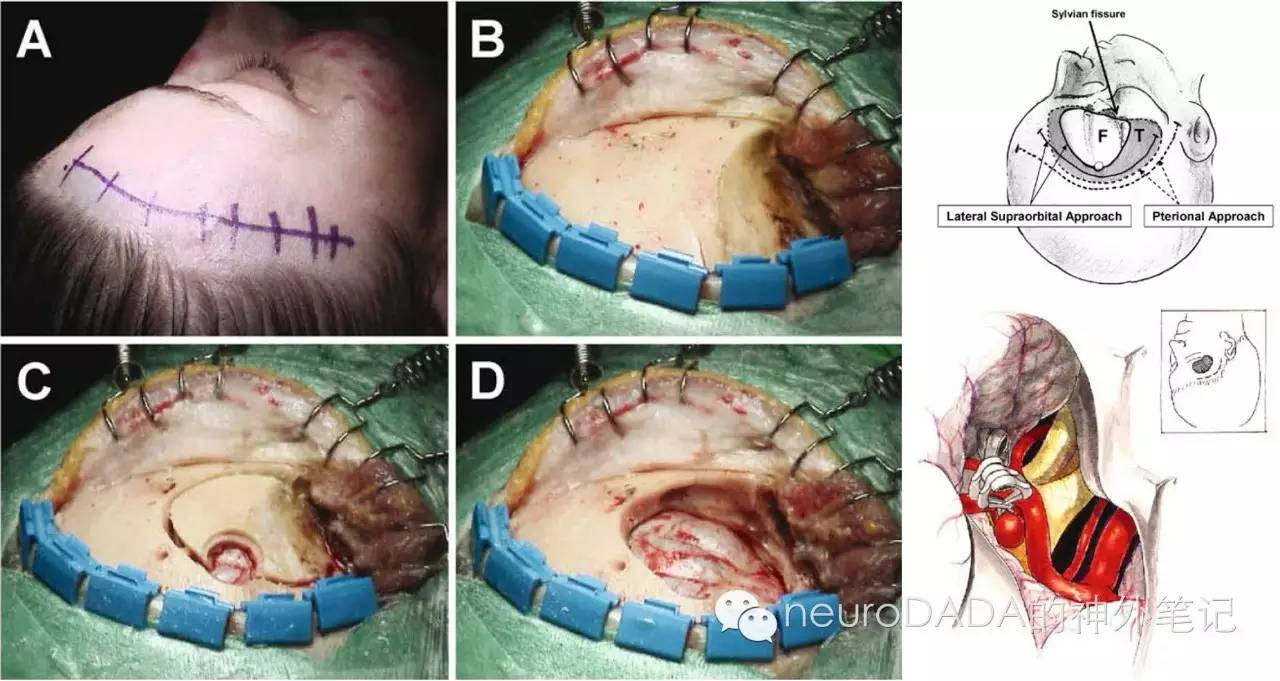
图12
小结
从上面的演变过程就可以看出,如今的翼点入路是由最初的额下入路移向侧方而来的,经Yasargil的完善,翼点入路如今的标准,应包括额颞开颅、蝶骨嵴的磨除、侧裂的开放。在此基础上,为处理更深的颅底区域,翼点入路存在着不同的扩展,如结合颞下入路扩展侧方视野;附加切除眶颧扩展上方视野;结合前床突的磨除彻底开放海绵窦。另一种相反的趋势则是继续做小,这也体现了历史的趋势。另外,经侧裂还有其他的扩展术式,如经侧裂行选择性杏仁海马切除术等,这里尚未涉及。因此,翼点入路是神经外科医师最基本也是最重要的武器,是学习其他入路的基础。
主要参考资料:
1.Altay, T. and W.T. Couldwell, The frontotemporal (pterional) approach: an historical perspective. Neurosurgery, 2012. 71(2): p. 481-91; discussion 491-2.
2.《Keyhole Approaches in Neurosurgery》2008

