



![]()
药物溶栓和机械取栓是缺血性卒中的最有效治疗方法,伴随其日益普及,缺血再灌注损伤成为很多缺血性卒中患者和临床医师要面临的挑战。加利福尼亚大学的Atsushi Mizuma等综述神经系统缺血再灌注损伤的基础和临床进展,发表于2018年7月的Stroke杂志,全文翻译如下。

机械取栓时代靶向再灌注损伤
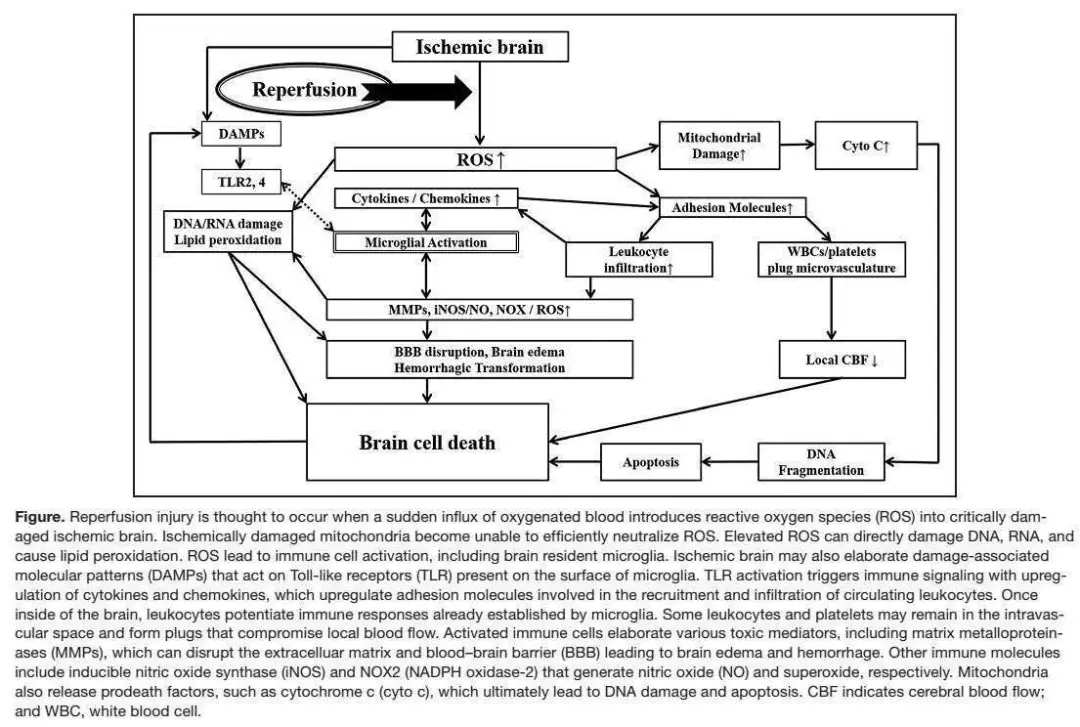
用r-tPA(recombinant tissue-type plasminogen activator)进行药物血管再通已成为急性缺血性脑卒中(IS)的主要治疗手段1。近期随机对照试验进一步证实机械取栓(MT)的价值2-4。虽然急性期治疗的主要目标是恢复血流,而如果再通太迟,与未恢复血流相比其损伤会更大5。这主要是由于产生过量的活性氧类(ROS),其可直接或通过触发炎症反应而间接损伤神经细胞。炎症导致产生损伤性免疫介质、效应分子和更多的ROS6。ROS也可通过DNA/RNA损伤和脂质过氧化引起细胞凋亡/坏死。这一循环称为再灌注损伤(R/I;见图)。
实验研究显示,相较于永久性大脑中动脉阻断(MCAO),>2-3小时的暂时性大脑中动脉阻断(tMCAO)可导致更加严重的后果7。在临床层面,延迟再通有时可导致更加不良的结局8。在某些患者,MRI上高信号急性再灌注标志与出血转化(HTf)和临床恶化相关,提示人类存在R/I9。因此,血管再通后针对R/I的辅助治疗可改善患者结局并减少r-tPA的并发症。
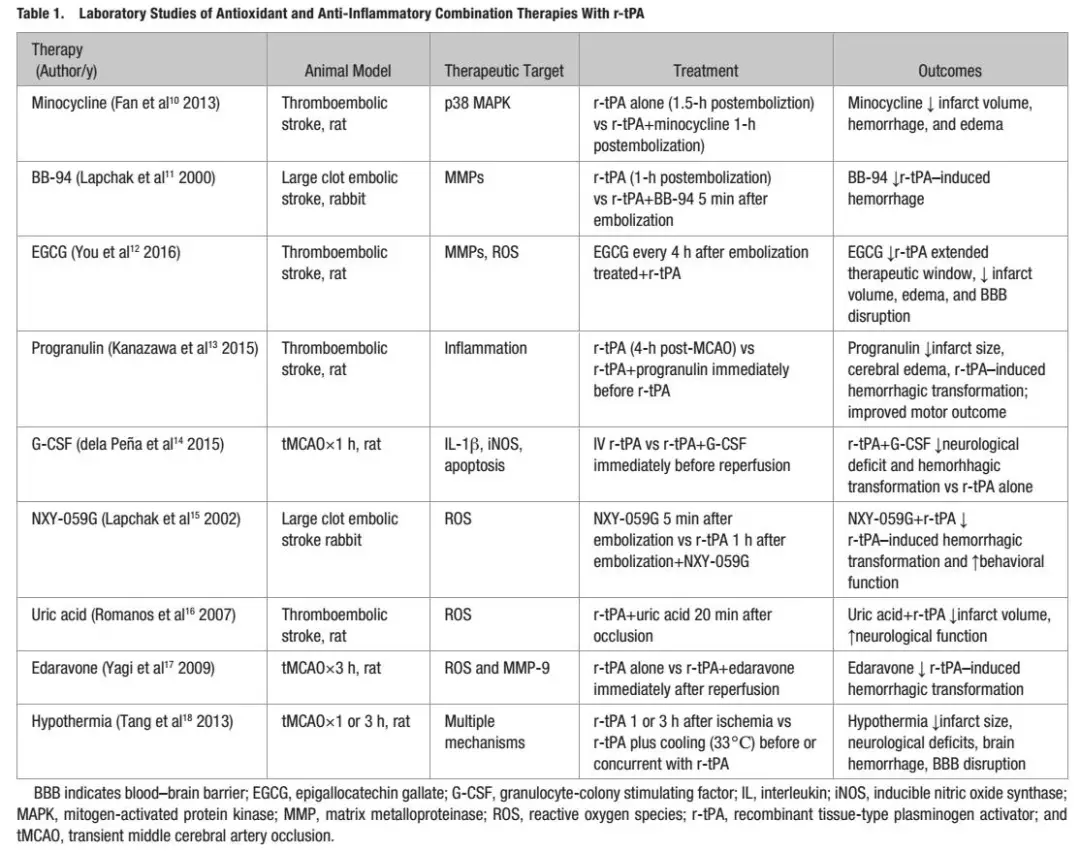
笔者将聚焦R/I的潜在机制和针对实验性血管再通模型中这些机制的实验室研究(如tMCAO或血栓栓塞性卒中)(表1)10-18。同时我们也会综述一下过去和现今的相关临床试验,有些与血管再通联合应用(表2)19-30。

R/I的抗炎治疗
卒中后炎症反应被认为会加重缺血损伤。可导致恶化的免疫分子包括炎症细胞因子、化学因子和免疫细胞产生的活性成分。脑细胞缺血损伤后,免疫细胞激活首先发生于小胶质细胞并释放免疫分子。随后,白细胞激活并浸润脑组织。一些实验室研究显示,阻止白细胞浸润可改善卒中模型的结局,虽然其临床效果尚未被证实31。
卒中后即出现炎症反应,因缺血性脑细胞会导致分泌一系列分子,这些分子统称为损伤相关分子模式。这些分子包括高迁移率簇蛋白B,过氧化物酶,嘌呤类,核苷酸类(包括ATP和UDP)和核酸片段6,31。损伤相关分子模式结合小胶质细胞和白细胞上的固有免疫受体(如Toll样和嘌呤受体),使其激活,然后激活炎性转录因子(核因子-κB和丝裂原活化蛋白激酶)。这些因子缺乏或药物将其阻断可显著保护卒中的实验动物32,33。这些因子可促进细胞因子,化学因子,黏附分子,基质金属蛋白-9(MMP-9),诱导型一氧化氮合酶和NADPH氧化酶(NOX)的产生,加重缺血损伤。促炎细胞因子白细胞介素(IL)-1β的影响可远及细胞翻译层面。

在一项II期临床试验,人类重组IL-1受体拮抗剂(IL-1β的内源性抑制剂)减少了梗塞体积并改善3个月的神经系统结局34。T细胞释放的促炎细胞因子(干扰素γ,IL-17,和IL-23)近期正作为治疗靶标研究。IL-17促进肿瘤坏死因子-α(TNF-α),IL-1β和MMP-9的表达,而IL-23则诱导IL-17的表达35。抑制这些细胞因子可改善实验R/I模型的神经系统结局。
在tMCAO后,小胶质细胞/巨噬细胞表达TNF-α诱导型蛋白8-样分子2,可起到抗炎作用。而TNF-α诱导型蛋白8-样分子2缺失型小鼠在tMCAO后则加重神经系统结局和炎症反应36。IL-10,IL-4和转化生长因子-β1是抗炎细胞因子,在卒中模型中均似与神经系统结局改善相关6,37。MMP-9由免疫细胞表达,可通过破坏血脑屏障(BBB)促进炎症反应。另外,内源性tPA激活纤溶酶,并进一步激活MMP-9。因此,应用r-tPA可能促进出血,如果入脑还可导致脑水肿,而MMP-9则成为一个相关治疗靶标38。
一些抗炎疗法已经在卒中模型中应用,尤其是与r-tPA联用。米诺环素具有多重抗细胞死亡效应,可改善神经系统结局并降低r-tPA相关的HTf10。米诺环素保护作用的一个机制可能是其通过阻断P38丝裂原活化蛋白激酶抑制小胶质细胞激活的能力。米诺环素也能通过抑制MMP改善BBB的完整性39。BB-94是一个MMP-9抑制剂,可降低兔卒中模型中r-tPA诱导的HTf11。然而,MMPs参与神经血管重塑,长期抑制可能阻碍修复作用40。表没食子儿茶素没食子酸酯(在绿茶中发现)因其抗氧化和神经保护特性而受到关注。
在卒中模型,表没食子儿茶素没食子酸酯下调MMP-2和MMP-9,同时上调纤溶酶原激活物抑制剂-112。没食子儿茶素没食子酸酯与r-tPA联用可延长r-tPA的治疗时间窗并减少脑水肿和BBB破坏12。颗粒蛋白前体(脑内的一种生长因子)被认为有抗炎和血管保护作用,缺血性卒中后其在小胶质细胞和内皮细胞中显著增加13。r-tPA联合颗粒蛋白前体在卒中模型中显示出改善神经系统结局和减少脑出血与脑水肿的作用。粒细胞集落刺激因子可能通过抗炎作用而提供神经保护41。在一个tMCAO模型中,相较于单独应用r-tPA,联用粒细胞集落刺激因子可减少HTf并改善神经系统结局14。
R/I的抗氧化/氮化治疗
IS后的再灌注通过线粒体呼吸链和NOX诱发氧化应激。缺血的线粒体被再灌注后产生的ROS充填,但不能有效地将其中和。内源性抗氧化酶(超氧化物歧化酶、谷胱甘肽过氧化物酶和过氧化氢酶)的过表达已证实可改善实验性卒中的结局。过表达超氧化物歧化酶的转基因小鼠可显著减少实验tMCAO模型的卒中面积,而超氧化物歧化酶缺失型小鼠结局较差42。过表达其它内源性抗氧化剂,如谷胱甘肽过氧化物酶和过氧化氢酶,也有类似的神经保护作用43。在临床层面,依布硒啉(ebselen,一种谷胱甘肽过氧化物酶类似物)可改善起病6小时内IS患者的神经系统结局44。
免疫细胞通过NOX途径产生超氧化物,可加剧氧化应激45。抑制NOX显示可改善实验性卒中的结局45。但NOX也可能在高血糖诱导的卒中恶化中扮演重要角色。葡萄糖可通过磷酸己糖支路代谢,产生NADPH,为生成NOX提供底物。罗布麻宁是一种NOX抑制剂,可改善实验中高血糖性tMCAO的结局46,减少高血糖诱发性BBB破坏的恶化及r-tPA应用时的HTf47。
在过去这些年,还研究过其它相关治疗策略。自由基清除剂(如替拉扎特或NXY-059联合r-tPA)在实验性卒中均有效果15,但在临床研究中是阴性的48,49。PSD-95蛋白(postsynaptic density-95,突触后致密物-95)与N-甲基-D-门冬氨酸受体相关。其募集神经源性一氧化氮合成酶,从而产生神经毒性一氧化氮50。PSD-95抑制剂NA-1可改善实验性R/I的结局。胰岛素样生长因子是一种参与促存活信号通路的多效能肽,也可抑制氧化与氮化应激51。尿酸通过抗氧化作用改善血栓栓塞卒中模型的结局16。依达拉奉是ROS清除剂,与r-tPA联用也可改善实验模型的神经系统结局17,在日本用于临床急性IS的治疗19。
R/I的抗凋亡治疗
ROS介导的损伤引起细胞凋亡,可能与R/I尤为相关。因为凋亡需要消耗细胞能量储备以促进细胞死亡52。线粒体发起的凋亡称为内源性途径。此时,线粒体向胞浆释放细胞色素C,与凋亡蛋白酶激活因子1和procaspase-9形成凋亡体53。凋亡体激活caspase-9并激活效应分子caspase-3,促进DNA清除52。超氧化物歧化酶过表达小鼠在R/I时显示出凋亡减少和细胞色素C移位,阻断线粒体源性caspase激活剂和线粒体丝氨酸蛋白酶也能达到此效果54。
Bcl-2家族参与凋亡的分子包括BAX、BAD和BID,它们触发细胞色素C释放,而Bcl-2和Bcl-XL阻碍其释放52。改变这些分子的平衡利于抗凋亡亚型的形成,可改善实验卒中的结局。当死亡受体与其受体结合,启则动外源性凋亡途径。研究广泛的受体-配体组合是Fas/FasL。FasL与Fas结合,激活caspase-8,最终激活caspase-3并清除DNA52。具有Fas突变的小鼠可少受R/I损害55。
最后,雌激素已知参与IS。与雄性动物相比,雌性动物在实验性卒中后结局更好。17-β雌二醇(E2)的保护作用可能与Bcl-2上调和抑制凋亡有关56。因此,性别特异性类固醇可能与凋亡调节关联。
与血流再通联合治疗的临床研究
虽然已经在实验卒中模型中研究了一些药物与r-tPA联用预防R/I,也有临床研究进行联用r-tPA和MT的探索。虽然没有刻意针对预防R/I设计,这些研究可为未来相关研究提供框架。
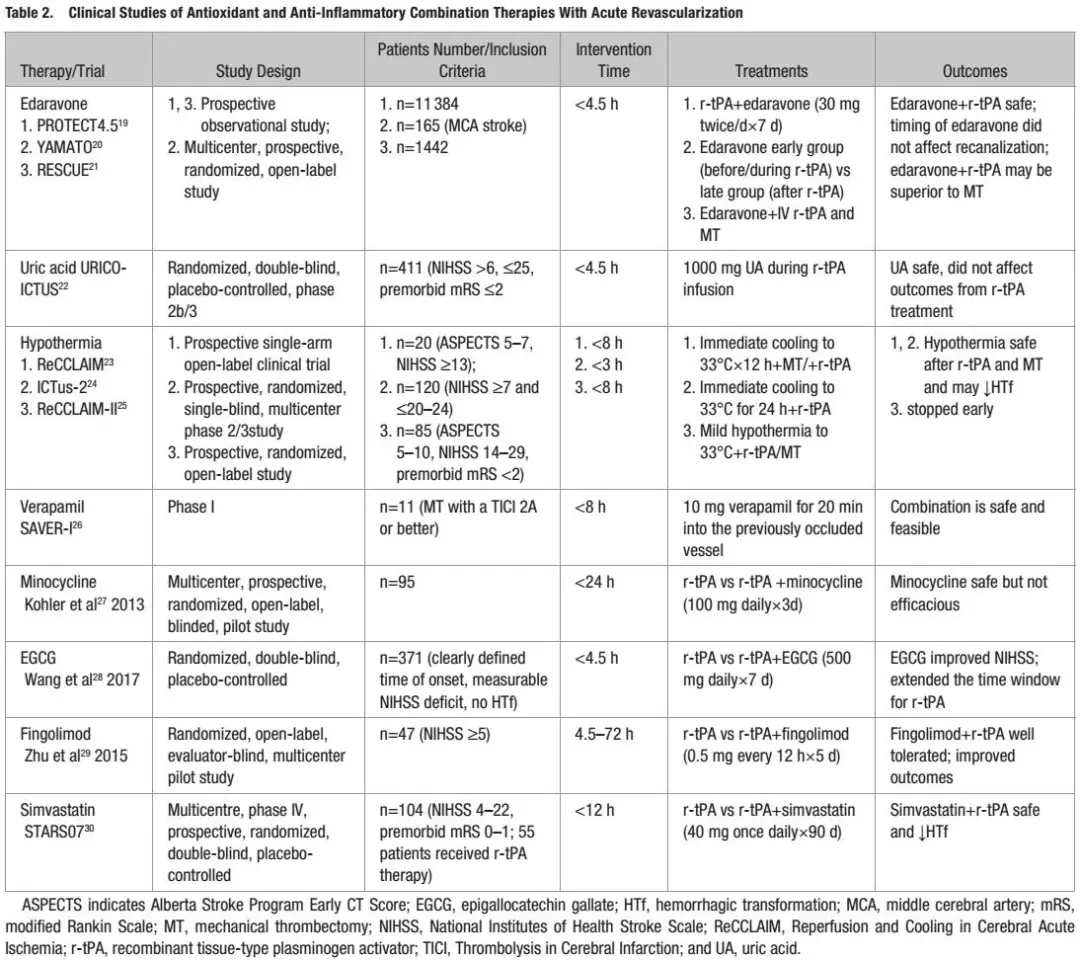
依达拉奉联合r-tPA/MT已经在日本用于临床。虽然缺乏对照组,2个观察性研究具有提示作用。PROTECT4.5(Post-marketing Registry on Treatment With Edaravone in Acute Cerebral Infarction by the Time Window of 4.5 Hours)评价依达拉奉联用r-tPA,提示这一组合可能增加较好结局的机会,减少HTf19。YAMATO(Tissue-Type Plasminogen Activator and Edaravone Combination Therapy)提示,应用r-tPA后,良好结局与依达拉奉应用的时机无关20。最后,对一项卒中注册实验(RESCUE Japan Registry[Recovery by Endovascular Salvage for Cerebral Ultra-Acute Embolism])的亚类分析提示,依达拉奉联用r-tPA比MT更有效21。
URICO-ICTUS(Efficacy Study of Combined Treatment With Uric Acid and r-tPA in Acute Ischemic Stroke)实验评价尿酸联用r-tPA/MT对急性IS的治疗效果,确定在发病4.5小时的时间窗内是安全的。此研究也报告,尿酸降低梗塞发展,改善早期再通和高血糖患者的结局16。有研究也证实了尿酸联用MT的有效性22。
治疗性亚低温,被认为可靶向多种R/I机制,也显示可改善心脏骤停和新生儿缺血缺氧的神经功能结局57。在实验性tMCAO,治疗性亚低温与r-tPA联用可减少BBB破坏和HTf18。ReCCLAIM(Reperfusion and Cooling in Cerebral Acute Ischemia)23和ICTuS-2(Intravascular Cooling in the Treatment of Stroke 2)24检验卒中患者中这种治疗组合,均显示这种治疗组合是安全可行的,尽管RECCLAIM-Ⅱ(进一步检验MT)因为缺乏资金支持而提前终止25。MT与经动脉内注入冷盐水联用而选择性脑降温的初步研究正在进行,显示是安全可行的58。
ACTION-1(Effect of Natalizumab on Infarct Volume in Acute Ischemia Stroke)研究那他珠单抗在急性IS中的安全和有效性。那他珠单抗是整合素α4的抗体,用于治疗多发性硬化。那他珠单抗被认为可减少淋巴细胞浸润和黏附分子上调。虽然那他珠单抗在实验性卒中未显示有效性59,ACTION-1包含接受r-tPA的患者60。虽然给那他珠单抗后梗塞体积无显著差异,但神经系统结局有改善。
其它的抗炎和抗氧化药物(均在临床上用于其它适应症)也在临床上与r-tPA联用。Ⅰ期实验SAVER-1(Superselective Administration of VErapamil During Recanalization in Acute Ischemic Stroke)研究维拉帕米联合r-tPA/MT的治疗效果,发现此组合安全26。类似的,米诺环素联用r-tPA也看起来是安全的,虽然效果不明确27。表没食子儿茶素没食子酸酯联用r-tPA看起来可延长r-tPA的治疗时间窗并改善结局28。一项小型研究提示,口服芬戈莫德能安全地改善90天神经功能结局61。同时,一项芬戈莫德联用r-tPA的初步研究证实,其安全和趋向良好临床结局,减少HTf29。近期,Ⅳ期实验STARS07(Stroke Treatment with Acute Reperfusion and Simvastatin)证实了辛伐他汀在治疗急性卒中的有效性和安全性,显示辛伐他汀联用r-tPA安全且可减少HTf30。
目前,有几项正在进行的旨在评价血管再通联合神经保护安全性和有效性的研究。与先前实验相比,这些研究直接检验辅助治疗联合r-tPA/MT是否改善结局,同时也可以研究R/I。活化蛋白C被认为可抑制炎症并阻止BBB破坏,在RHAPSODY(The Safety Evaluation of 3K3A-activated protein C in Ischemic Stroke)(NCT02222714)中正与r-tPA/MT联合应用62。
另一项阿托伐他汀与MT联用的临床研究SEATIS(The Safety and Efficacy Study of High Dose Atorvastatin After Thrombolytic Treatment in Acute Ischemic Stroke)(NCT02452502)也在进行中63。NA-1联合MT的ESCAPE-NA1(Safety and Efficacy of NA-1 in Subjects Undergoing Endovascular Thrombectomy for Stroke)(NCT02930018)旨在评价安全性和有效性。虽然并未限制招募接受r-tPA/MT治疗的患者,ACTIONⅡ(NCT02730455)评价静脉用那他珠单抗的安全性和有效性。
最后,FAMTAIS(Fingolimod with Alteplase bridging with Mechanical Thrombectomy in Acute Ischemic Stroke;NCT02956200)作为一项Ⅱ期桥接疗法(fingolimod联合r-tPA/MT),近期开始评估在大血管堵塞中的安全性和有效性64。
结论
对急性卒中R/I的广泛研究有可能找到可向临床转化的潜在治疗靶点。R/I现象在实验室已经有较好的研究。虽然在临床上不清楚,急性血管再通的新进展可能帮助明确人类是否存在R/I。尽管药物溶栓有增加脑出血的风险,针对同一靶标的辅助治疗在实验条件下可减少HTf,延长治疗时间窗和改善结局。我们推测这些治疗也能使更多的卒中患者适合血管再通治疗。
侯坤,吉林大学第一医院神经外科
李桂晨,吉林大学第一医院神经内科
参考文献
1. Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2014;CD000213.
2. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al; HERMES Collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from fie randomised trials. Lancet. 2016;387:1723–1731.doi: 10.1016/S0140-6736(16)00163-X.
3. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al; DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between defiit and infarct. N Engl J Med. 2018;378:11–21. doi: 10.1056/NEJMoa1706442.
4. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, OrtegaGutierrez S, et al; DEFUSE 3 Investigators. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med.
2018;378:708–718. doi: 10.1056/NEJMoa1713973.
5. Aronowski J, Strong R, Grotta JC. Reperfusion injury: demonstration of brain damage produced by reperfusion after transient focal ischemia in rats. J Cereb Blood Flow Metab. 1997;17:1048–1056. doi: 10.1097/00004647-199710000-00006.
6. Amantea D, Micieli G, Tassorelli C, Cuartero MI, Ballesteros I, Certo M, et al. Rational modulation of the innate immune system for neuroprotection in ischemic stroke. Front Neurosci. 2015;9:147. doi: 10.3389/fnins.2015.00147.
7. Yang GY, Betz AL. Reperfusion-induced injury to the blood-brain barrier after middle cerebral artery occlusion in rats. Stroke. 1994;25:1658–1664; discussion 1664.
8. Lees KR, Bluhmki E, von Kummer R, Brott TG, Toni D, Grotta JC, et al; ECASS, ATLANTIS, NINDS and EPITHET rt-PA Study Group. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695–1703. doi: 10.1016/S0140-6736(10)60491-6.
9. Warach S, Latour LL. Evidence of reperfusion injury, exacerbated by thrombolytic therapy, in human focal brain ischemia using a novel imaging marker of early blood-brain barrier disruption. Stroke.2004;35(11 suppl 1):2659–2661. doi: 10.1161/01.STR.0000144051.32131.09.
10. Fan X, Lo EH, Wang X. Effects of minocycline plus tissue plasminogen activator combination therapy after focal embolic stroke in type 1 diabetic rats. Stroke. 2013;44:745–752. doi: 10.1161/STROKEAHA.111.000309.
11. Lapchak PA, Chapman DF, Zivin JA. Metalloproteinase inhibition reduces thrombolytic (tissue plasminogen activator)-induced hemorrhage after thromboembolic stroke. Stroke. 2000;31:3034–3040.
12. You YP. Epigallocatechin gallate extends the therapeutic window of recombinant tissue plasminogen activator treatment in ischemic rats. J Stroke Cerebrovasc Dis. 2016;25:990–997. doi: 10.1016/j.jstrokecerebrovasdis.2016.01.014.
13. Kanazawa M, Kawamura K, Takahashi T, Miura M, Tanaka Y, Koyama M, et al. Multiple therapeutic effects of progranulin on experimental acute ischaemic stroke. Brain. 2015;138(pt 7):1932–1948. doi:10.1093/brain/awv079.
14. dela Peña IC, Yoo A, Tajiri N, Acosta SA, Ji X, Kaneko Y, et al. Granulocyte colony-stimulating factor attenuates delayed tPA-induced hemorrhagic transformation in ischemic stroke rats by enhancing angiogenesis and vasculogenesis. J Cereb Blood Flow Metab. 2015;35:338–346. doi: 10.1038/jcbfm.2014.208.
15. Lapchak PA, Araujo DM, Song D, Wei J, Purdy R, Zivin JA. Effects of the spin trap agent disodium- [tert-butylimino)methyl]benzene-1,3-disulfonate N-oxide (generic NXY-059) on intracerebral hemorrhage in a rabbit large clot embolic stroke model: combination studies with tissue plasminogen activator. Stroke. 2002;33:1665–1670.
16. Romanos E, Planas AM, Amaro S, Chamorro A. Uric acid reduces brain damage and improves the benefis of rt-PA in a rat model of thromboembolic stroke. J Cereb Blood Flow Metab. 2007;27:14–20. doi: 10.1038/sj.jcbfm.9600312.
17. Yagi K, Kitazato KT, Uno M, Tada Y, Kinouchi T, Shimada K, et al. Edaravone, a free radical scavenger, inhibits MMP-9-related brain hemorrhage in rats treated with tissue plasminogen activator. Stroke. 2009;40:626–631. doi: 10.1161/STROKEAHA.108.520262.
18. Tang XN, Liu L, Koike MA, Yenari MA. Mild hypothermia reduces tissue plasminogen activator-related hemorrhage and blood brain barrier disruption after experimental stroke. Ther Hypothermia Temp Manag. 2013;3:74–83. doi: 10.1089/ther.2013.0010.
19. Yamaguchi T, Awano H, Matsuda H, Tanahashi N; PROTECT4.5 Investigators. Edaravone with and without.6 Mg/Kg alteplase within 4.5 hours after ischemic stroke: a prospective cohort study (PROTECT4.5). J Stroke Cerebrovasc Dis. 2017;26:756–765. doi: 10.1016/j.jstrokecerebrovasdis.2016.10.011.
20. Aoki J, Kimura K, Morita N, Harada M, Metoki N, Tateishi Y, et al;YAMATO Study Investigators. YAMATO Study (Tissue-type plasminogen activator and edaravone combination therapy). Stroke. 2017;48:712–719. doi: 10.1161/STROKEAHA.116.015042.
21. MiyajiY, Yoshimura S, Sakai N, Yamagami H, Egashira Y, Shirakawa M, et al. Effect of edaravone on favorable outcome in patients with acute cerebral large vessel occlusion: subanalysis of RESCUE-Japan Registry. Neurol Med Chir (Tokyo). 2015;55:241–247. doi: 10.2176/nmc.ra.2014-0219.
22. Amaro S, Llull L, Renú A, Laredo C, Perez B, Vila E, et al. Uric acid improves glucose-driven oxidative stress in human ischemic stroke. Ann Neurol. 2015;77:775–783. doi: 10.1002/ana.24378.
23. Horn CM, Sun CH, Nogueira RG, Patel VN, Krishnan A, Glenn BA, et al. Endovascular Reperfusion and Cooling in Cerebral Acute Ischemia (ReCCLAIM I). J Neurointerv Surg. 2014;6:91–95. doi: 10.1136/neurintsurg-2013-010656.
24. Lyden P, Hemmen T, Grotta J, Rapp K, Ernstrom K, Rzesiewicz T, et al; Collaborators. Results of the ICTuS 2 Trial (Intravascular Cooling in the Treatment of Stroke 2). Stroke. 2016;47:2888–2895. doi: 10.1161/STROKEAHA.116.014200.
25. The Internet Stroke Center. REperfusion with Cooling in CerebraL Acute IscheMia II “RECCLAIM-II”. http://www.strokecenter.org/trials/clinicalstudies/reperfusion-with-cooling-in-cerebral-acute-ischemiaii–2. Accessed April 17, 2018.
26. Fraser JF, Maniskas M, Trout A, Lukins D, Parker L, Stafford WL, et al. Intra-arterial verapamil post-thrombectomy is feasible, safe, and neuroprotective in stroke. J Cereb Blood Flow Metab. 2017;37:3531–3543.doi: 10.1177/0271678X17705259.
27. Kohler E, Prentice DA, Bates TR, Hankey GJ, Claxton A, van Heerden J, et al. Intravenous minocycline in acute stroke: a randomized, controlled pilot study and meta-analysis. Stroke. 2013;44:2493–2499. doi:
10.1161/STROKEAHA.113.000780.
28. Wang XH, You YP. Epigallocatechin gallate extends therapeutic window of recombinant tissue plasminogen activator treatment for brain ischemic stroke: a randomized double-blind and placebo-controlled trial. Clin Neuropharmacol. 2017;40:24–28. doi:10.1097/WNF.0000000000000197.
29. Zhu Z, Fu Y, Tian D, Sun N, Han W, Chang G, et al. Combination of the immune modulator figolimod with alteplase in acute ischemic stroke: a pilot trial. Circulation. 2015;132:1104–1112. doi: 10.1161/CIRCULATIONAHA.115.016371.
30. Montaner J, Bustamante A, García-Matas S, Martínez-Zabaleta M, Jiménez C, de la Torre J, et al; STARS Investigators. Combination of thrombolysis and statins in acute stroke is safe: results of the STARS randomized trial (Stroke Treatment With Acute Reperfusion and Simvastatin). Stroke. 2016;47:2870–2873. doi: 10.1161/STROKEAHA.116.014600.
31. Danton GH, Dietrich WD. Inflmmatory mechanisms after ischemia and stroke. J Neuropathol Exp Neurol. 2003;62:127–136.
32. Harari OA, Liao JK. NF-κB and innate immunity in ischemic stroke. Ann N Y Acad Sci. 2010;1207:32–40. doi: 10.1111/j.1749-6632.2010.05735.x.
33. Sun J, Nan G. The mitogen-activated protein kinase (MAPK) signaling pathway as a discovery target in stroke. J Mol Neurosci. 2016;59:90–98. doi: 10.1007/s12031-016-0717-8.
34. Emsley HC, Smith CJ, Georgiou RF, Vail A, Hopkins SJ, Rothwell NJ,
et al; Acute Stroke Investigators. A randomised phase II study of interleukin-1 receptor antagonist in acute stroke patients. J Neurol Neurosurg Psychiatry. 2005;76:1366–1372. doi: 10.1136/jnnp.2004.054882.
35. Yago T, Nanke Y, Kawamoto M, Furuya T, Kobashigawa T, Kamatani N, et al. IL-23 induces human osteoclastogenesis via IL-17 in vitro, and anti-IL-23 antibody attenuates collagen-induced arthritis in rats. Arthritis Res Ther. 2007;9:R96. doi: 10.1186/ar2297.
36. Zhang Y, Wei X, Liu L, Liu S, Wang Z, Zhang B, et al. TIPE2, a novel regulator of immunity, protects against experimental stroke. J Biol Chem. 2012;287:32546–32555. doi: 10.1074/jbc.M112.348755.
37. Zhao X, Wang H, Sun G, Zhang J, Edwards NJ, Aronowski J. Neuronal interleukin-4 as a modulator of microglial pathways and ischemic brain damage. J Neurosci. 2015;35:11281–11291. doi: 10.1523/JNEUROSCI.1685-15.2015.
38. Chaturvedi M, Kaczmarek L. MMP-9 inhibition: a therapeutic strategy in ischemic stroke. Mol Neurobiol. 2014;49:563–573. doi: 10.1007/s12035-013-8538-z.
39. Machado LS, Kozak A, Ergul A, Hess DC, Borlongan CV, Fagan SC. Delayed minocycline inhibits ischemia-activated matrix metalloproteinases 2 and 9 after experimental stroke. BMC Neurosci. 2006;7:56. doi:10.1186/1471-2202-7-56.
40. Yang Y, Rosenberg GA. Matrix metalloproteinases as therapeutic targets for stroke. Brain Res. 2015;1623:30–38. doi: 10.1016/j.brainres.2015.04.024.
41. Abe K, Yamashita T, Takizawa S, Kuroda S, Kinouchi H, Kawahara N. Stem cell therapy for cerebral ischemia: from basic science to clinical applications. J Cereb Blood Flow Metab. 2012;32:1317–1331. doi: 10.1038/jcbfm.2011.187.
42. Niizuma K, Endo H, Chan PH. Oxidative stress and mitochondrial dysfunction as determinants of ischemic neuronal death and survival. J Neurochem. 2009;109(suppl 1):133–138. doi: 10.1111/j.1471-4159.2009.05897.x.
43. Armogida M, Nisticò R, Mercuri NB. Therapeutic potential of targeting hydrogen peroxide metabolism in the treatment of brain ischaemia. Br J Pharmacol. 2012;166:1211–1224. doi: 10.1111/j.1476-5381.2012.01912.x.
44. Ogawa A, Yoshimoto T, Kikuchi H, Sano K, Saito I, Yamaguchi T, et al. Ebselen in acute middle cerebral artery occlusion: a placebo-controlled, double-blind clinical trial. Cerebrovasc Dis. 1999;9:112–118. doi: 10.1159/000015908.
45. Kahles T, Brandes RP. NADPH oxidases as therapeutic targets in ischemic stroke. Cell Mol Life Sci. 2012;69:2345–2363. doi: 10.1007/s00018-012-1011-8.
46. Suh SW, Shin BS, Ma H, Van Hoecke M, Brennan AM, Yenari MA, et al. Glucose and NADPH oxidase drive neuronal superoxide formation in stroke. Ann Neurol. 2008;64:654–663. doi: 10.1002/ana.21511.
47. Won SJ, Tang XN, Suh SW, Yenari MA, Swanson RA. Hyperglycemia promotes tissue plasminogen activator-induced hemorrhage by increasing superoxide production. Ann Neurol. 2011;70:583–590. doi:10.1002/ana.22538.
48. Chamorro Á, Dirnagl U, Urra X, Planas AM. Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and inflmmation. Lancet Neurol. 2016;15:869–881. doi: 10.1016/S1474-4422(16)00114-9.
49. Green AR, Ashwood T. Free radical trapping as a therapeutic approach to neuroprotection in stroke: experimental and clinical studies with NXY-059 and free radical scavengers. Curr Drug Targets CNS Neurol Disord. 2005;4:109–118.
50. Instrum R, Sun HS. Restoring neuroprotection through a new preclinical paradigm: translational success for NA-1 in stroke therapy. Acta Pharmacol Sin. 2013;34:3–5. doi: 10.1038/aps.2012.175.
51. Kooijman R, Sarre S, Michotte Y, De Keyser J. Insulin-like growth factor I: a potential neuroprotective compound for the treatment of acute ischemic stroke? Stroke. 2009;40:e83–e88. doi: 10.1161/STROKEAHA.108.528356.
52. Broughton BR, Reutens DC, Sobey CG. Apoptotic mechanisms after cerebral ischemia. Stroke. 2009;40:e331–e339. doi: 10.1161/STROKEAHA.108.531632.
53. Fujimura M, Morita-FujimuraY, Noshita N, Sugawara T, Kawase M, Chan PH. The cytosolic antioxidant copper/zinc-superoxide dismutase prevents the early release of mitochondrial cytochrome c in ischemic brain after transient focal cerebral ischemia in mice. J Neurosci. 2000;20:2817–2824.
54. Althaus J, Siegelin MD, Dehghani F, Cilenti L, Zervos AS, Rami A. The serine protease Omi/HtrA2 is involved in XIAP cleavage and in neuronal cell death following focal cerebral ischemia/reperfusion. Neurochem Int.2007;50:172–180. doi: 10.1016/j.neuint.2006.07.018.
55. Rosenbaum DM, Gupta G, D’Amore J, Singh M, Weidenheim K, Zhang H, et al. Fas (CD95/APO-1) plays a role in the pathophysiology of focal cerebral ischemia. J Neurosci Res. 2000;61:686–692. doi: 10.1002/1097-4547(20000915)61:6<686::AID-JNR12>3.0.CO;2-7.
56. Cardona-Gómez GP, Mendez P, DonCarlos LL, Azcoitia I, Garcia-Segura LM. Interactions of estrogens and insulin-like growth factor-I in the brain:implications for neuroprotection. Brain Res Brain Res Rev. 2001;37:320–334.
57. Yenari MA, Han HS. Neuroprotective mechanisms of hypothermia in brain ischaemia. Nat Rev Neurosci. 2012;13:267–278. doi: 10.1038/nrn3174.
58. ChenJ, Liu L, Zhang H, Geng X, Jiao L, Li G, et al. Endovascular hypothermia in acute ischemic stroke: pilot study of selective intra-arterial cold saline infusion. Stroke. 2016;47:1933–1935. doi: 10.1161/STROKEAHA.116.012727.
59. Langhauser F, Kraft P, Göb E, Leinweber J, Schuhmann MK, Lorenz K, et al. Blocking of α4 integrin does not protect from acute ischemic stroke in mice. Stroke. 2014;45:1799–1806. doi: 10.1161/STROKEAHA.114.005000.
60. Elkins J, Veltkamp R, Montaner J, Johnston SC, Singhal AB, Becker K, et al. Safety and effiacy of natalizumab in patients with acute ischaemic stroke (ACTION): a randomised, placebo-controlled, double-blind phase 2 trial. Lancet Neurol. 2017;16:217–226. doi: 10.1016/S1474-4422(16)30357-X.
61. Fu Y, Zhang N, Ren L, Yan Y, Sun N, Li YJ, et al. Impact of an immune modulator figolimod on acute ischemic stroke. Proc Natl Acad Sci USA.2014;111:18315–18320. doi: 10.1073/pnas.1416166111.
62. Amar AP, Griffi JH, Zlokovic BV. Combined neurothrombectomy or thrombolysis with adjunctive delivery of 3K3A-activated protein C in acute ischemic stroke. Front Cell Neurosci. 2015;9:344. doi: 10.3389/fncel.2015.00344.
63. Cimino M, Gelosa P, Gianella A, Nobili E, Tremoli E, Sironi L. Statins:multiple mechanisms of action in the ischemic brain. Neuroscientist. 2007;13:208–213. doi: 10.1177/1073858406297121.
64. Zhang S, Zhou Y, Zhang R, Zhang M, Campbell B, Lin L, et al. Rationale and design of combination of an immune modulator figolimod with alteplase bridging with mechanical thrombectomy in acute ischemic stroke (FAMTAIS) trial. Int J Stroke. 2017;12:906–909. doi: 10.1177/1747493017710340.
![]()
