


Our case
History
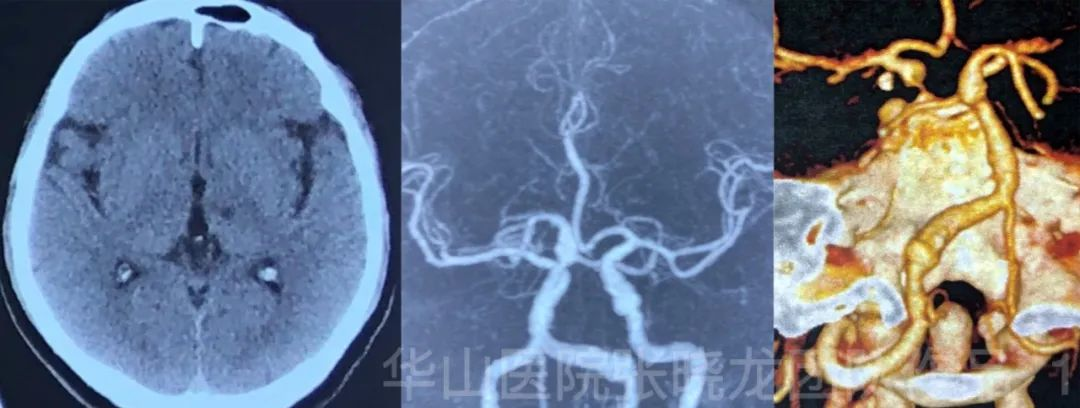
Figure 1. CT shows the lacunar infarction of left thalamus. CTA images show left vertebral-basilar artery and ICA dissections/dissecting aneurysms, indicating the possibility of angio dysplasia. 图 1. CT显示左侧丘脑腔隙性梗死。CTA显示左侧椎-基底动脉和颈内动脉夹层/夹层动脉瘤,血管发育不良。

Figure 2. High resolution MRI shows left vertebra artery dissection with intimal flap and abnormal vessel wall enhancement. 图 2. 高分辨率MRI显示左侧椎动脉夹层和内膜瓣,以及血管壁的异常强化。
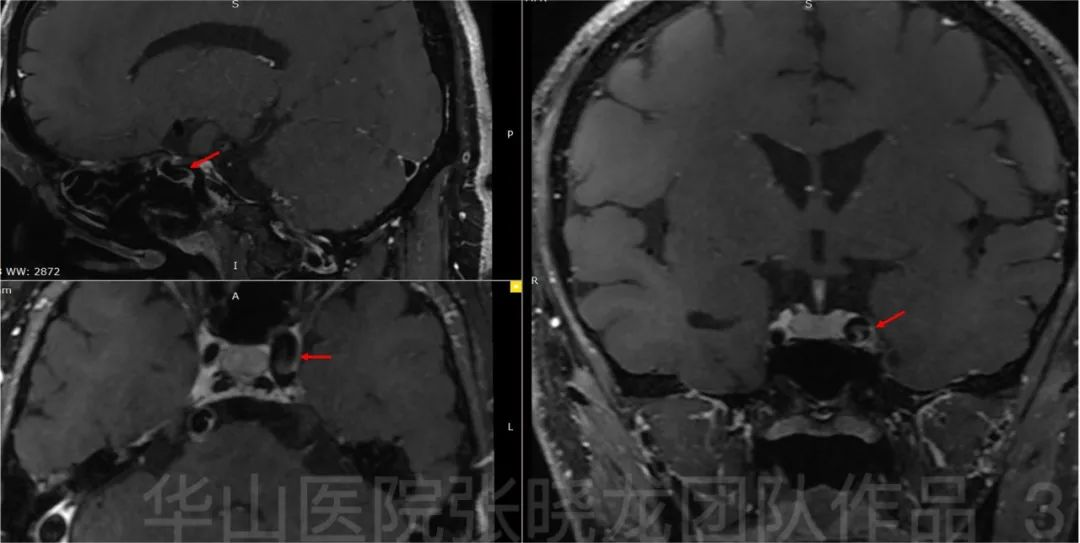
Figure 3. High resolution MRI shows left carotid artery dilation with intimal flap enhancement, indication the diagnose of dissection. 图 3. 高分辨率MRI显示左侧颈动脉扩张和内膜瓣强化,提示动脉夹层。
1
Treatment strategy
•左侧椎动脉V4段夹层动脉瘤:高分辨率MRI显示左侧椎动脉扩张段血管壁异常强化,提示可用大圈辅助支架技术重塑血管壁。
Video 2. General heparinization. 8F guide catheter and Navien (115cm) were placed in the left V4.Headway 21 was placed in the right P2. LVIS 5.5mm*20mm stent was deployed covering BA dissection.视频 2. 全身肝素化。8F导管和Navien(115cm)导管置于左侧V4段。Headway 21微导管置于右侧P2段。置入LVIS 5.5mm*20mm支架覆盖基底动脉夹层。

Figure 4. Echelon-10 microcatheter was sent to the left V4 aneurysm sac. Two Microplex-10 7mm*30cm coils were inserted. The coil loops were inserted loosely and evenly in the distal segment.图 4. 将Echelon-10微导管送入左侧V4段动脉瘤腔内。填入两枚Microplex-10 7mm*30cm弹簧圈。在其远端部分,弹簧圈应疏送而均匀地填入。
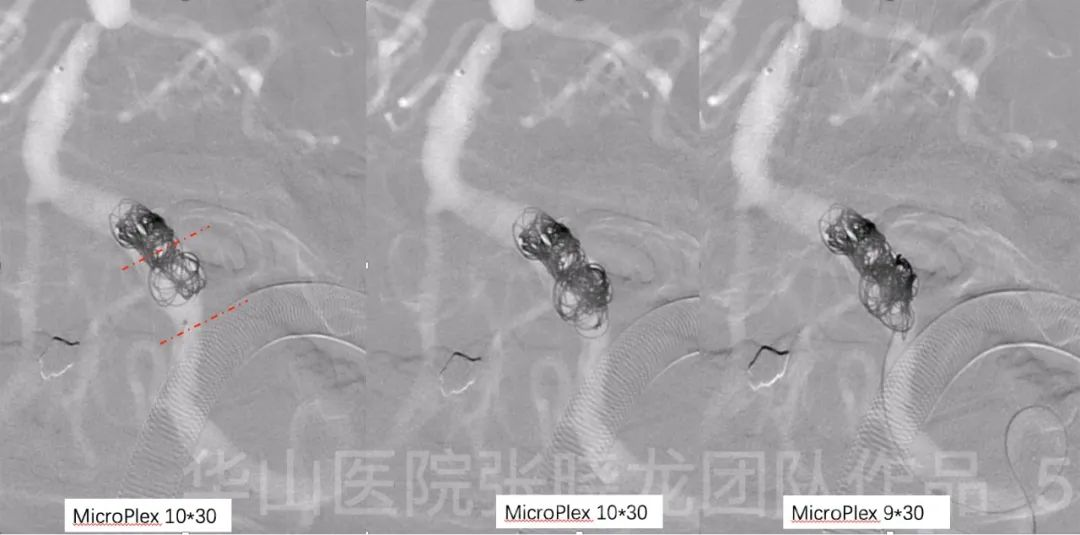
Figure 5. Two Microplex-10 10mm*30cm and a Microplex-10 9mm*30cm coils were inserted,embolizing the proximal segment of the aneurysm.图 5. 填入两枚Microplex-10 10mm*30cm和一枚Microplex-10 9mm*30cm弹簧圈栓塞动脉瘤近端。
Video 3. LVIS 5.5mm*20mm.
Figure 6. Solitaire 6mm*30mm.

Figure 7. Rotational angiography shows the intact of intracranial vessels.图 7. 旋转血管造影上颅内血管显示完整。
3
Post operation
• PE:GCS 15, no neurologic defict.
• Medication:Aspirin,Clopidogrel and Rosuvastatin.
• 查体:GCS15,无神经功能缺损症状。
• 药物:阿司匹林,氯吡格雷和瑞舒伐他汀。
4
Summary
Stenting is necessary for the basilar artery dissection. For the distal stenosis, balloon dilation may affect the right SCA.
From the high-resolution MR imaging, the left VA dissection segment contains an abnormal enhanced vessel wall, so large coil assisted stenting can reconstructand protect the vulnerable wall. Early treatment of the left vertebral-basilar artery dissecting aneurysm can avoid subsequent complicated treatment and mass effecton the brain stem.
Proper coil selection according to the diameter of the segment, loosely packing the left VA dissecting aneurysm and pushing the stent during deployment can allow the LVIS stent to fully expand. Also, the Solitaire stent with good radial support can reinforce the prior LVIS stent.
Right CCA, brachiocephalic trunk with subclavian artery dissections and stenosis can be followed up and later treated if necessary.
A flow diverter can be deployed if the dissecting aneurysm has recurred upon angiographic follow-up.
总结
基底动脉夹层需行支架成形术。对远端狭窄的球囊扩张可能累及右侧小脑上动脉。
高分辨率MRI显示左侧椎动脉夹层段存在异常强化的血管壁,因此大圈辅助支架技术可以重塑并保护脆弱的血管壁。左侧椎-基底动脉夹层动脉瘤的早期治疗可以避免后续的复杂治疗和脑干占位效应。
正确的弹簧圈选择要根据动脉瘤的直径。疏送栓塞左侧椎动脉夹层动脉瘤并在释放时推挤支架可令LVIS支架完全释放。此外,Solitaire支架具有良好的径向支撑作用,可加固先前的LVIS支架。
右侧颈总动脉、头臂干、锁骨下动脉夹层伴狭窄可继续随访,必要时再行手术治疗。
如果在随访血管造影中发现夹层动脉瘤复发可使用血流导向装置。
5
Four month follow up
• Decline of memory slightly aggravated than spanvious condition.
• PE(-)
• Medication:Aspirin,Clopidogrel and Rosuvastatin.
• 记忆力下降较前略有加重。
• 查体:阴性
• 药物:阿司匹林,氯吡格雷和瑞舒伐他汀。
Figure 8. Four month follow up angiography shows no relapse of the left V4 dissecting aneurysm with parent artery patent.图 8. GIF4个月随访血管造影未见左侧 V4段夹层动脉瘤复发,且载瘤动脉通畅。

Figure 9. Better reconstruction of left VA and BA after comparison with post-operative angiography.图 9. 与术后血管造影相比,左侧椎动脉、基底动脉血流重建效果更好。
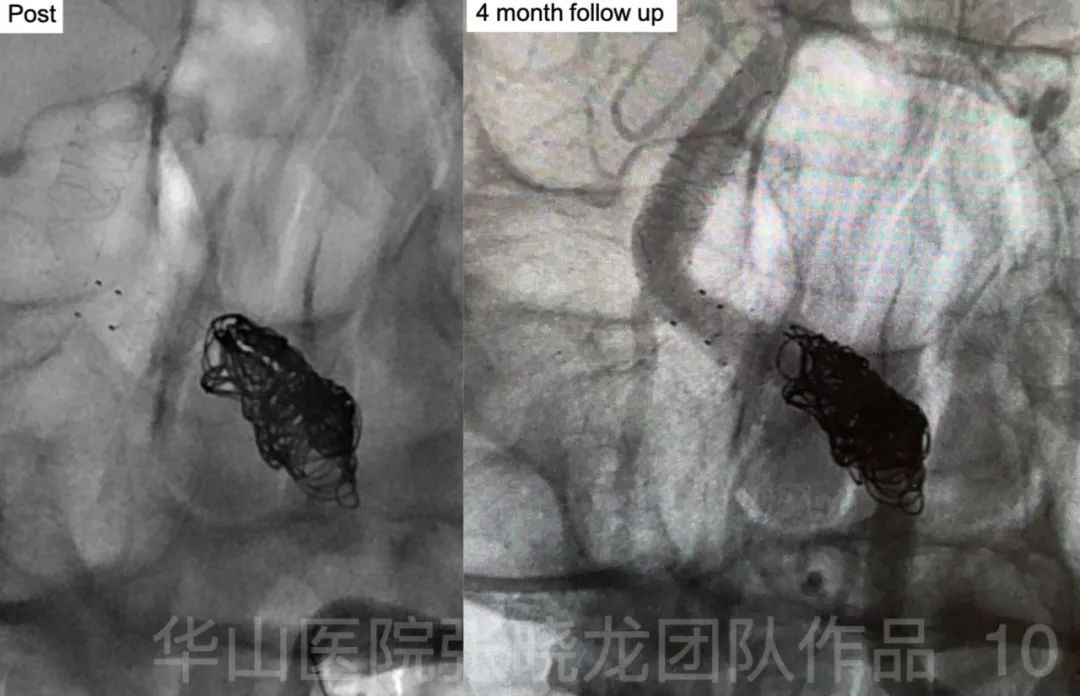
Figure 10. Four month follow up angiography shows better shaping of coils compared to post-operative angiography. 图 10. 与术后即刻造影相比,四月随访造影中弹簧圈形态更紧密。
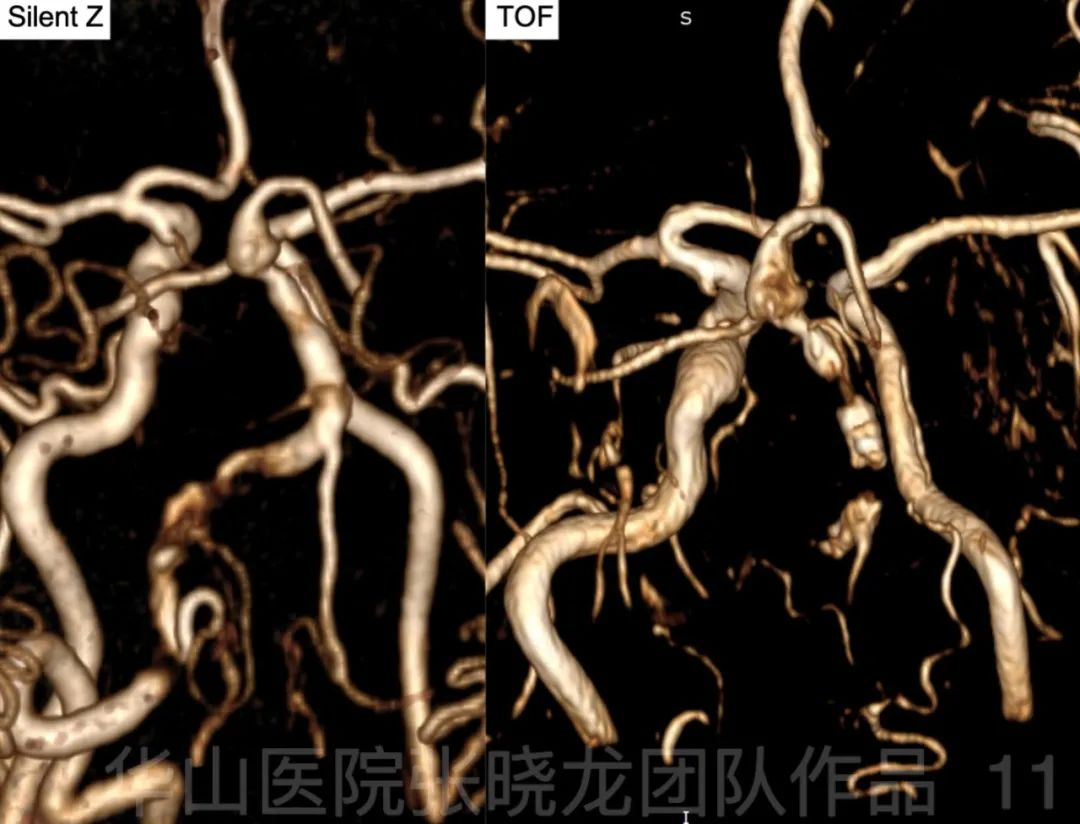
Figure 11. Post-stent vessel was showed well by Silent Z MR compared to 3D TOF MRA.图 11. Silent Z MR较3D TOF MRA能更好地显示支架置入后的血管。
Figure 12. Follow up HR MRI shows parent artery wall enhancement without intima flap. 图 12. 随访高分辨率MRI显示载瘤动脉管壁强化,未见内膜瓣。

Figure 13. Follow up angiography shows RCCA and LICA dissection kept stable.图 13. 随访血管造影显示右侧颈总动脉和左侧颈内动脉夹层保持稳定。
5
Follow up Summary
•HR MRI shows no evidence of the intima flap in left V4, indicating well reconstruction of dissections after stent assisted coiling. The enhancement of the parent artery and aneurysm wall is also seen.
•Right CCA, LICA, brachiocephalic trunk and subclavian artery dissections were stable which can be followed up. However, if the patient symptoms were aggravated,these lesions should be treated.
•Continue medication of Aspirin, Clopidogrel and Rosuvastatin.
•Follow up 1-2 year later was scheduled.
•高分辨率MRI上左侧V4段未见内膜瓣,说明支架辅助栓塞术后夹层重建良好。载瘤动脉及动脉瘤壁可见强化。
•右侧颈总动脉、左侧颈内动脉、头臂干及右锁骨下动脉夹层稳定,可继续随访。但是如果患者症状加重,这些病变应进行治疗。
•继续服用阿司匹林、氯吡格雷和瑞舒伐他汀。
•计划1-2年后随访。
![]()
